Colic - effects of inflammation
/
By Dr Zofia Lisowski, Prof. Scott Pirie & Dr Neil Hudson
Overview of colic
Colic is a term used to describe the display of abdominal pain in the horse. It is the most common emergency in horses with four to ten out of every 100 horses likely to experience at least one episode of colic each year. It is also the single most common cause of equine mortality. In the US, one study showed that thoroughbreds were more likely to develop colic1 than other breeds. It is of great welfare concern to horse owners, and with the estimated costs associated with colic in the US exceeding $115 million dollars per year2 and the average cost of a horse undergoing colic surgery that requires a resection in the UK being £6437.803, it is also a significant economic issue for horse owners.
Horses with abdominal pain show a wide range of clinical signs, ranging from flank watching and pawing the ground in mild cases, to rolling and being unable to remain standing for any significant period of time in more severe cases. There are numerous (over 50) specific causes of colic. In general, colic occurs as a result of disruption to the normal function of the gastrointestinal tract. This may be attributable to mechanical causes such as an obstruction (constipation), distension (excess gas) or a volvulus (twisted gut). It may also have a functional cause, whereby the intestine doesn’t work as normal in the absence of an associated mechanical problem; for example, equine grass sickness is associated with a functional derangement of intestinal motility due to loss of nerves within the intestine.

Management of colic depends on the cause and can necessitate either a medical or surgical approach. Most horses with colic will either improve spontaneously or with simple medical treatment alone; however, a significant proportion may need more intensive medical treatment or surgery. Fortunately, due to improvements in surgical techniques and post-operative management, outcomes of colic surgery have improved over the past few decades with up to 85% of horses surviving to discharge. Crucially for the equine thoroughbred racehorse population, several studies focussed on racehorses that had undergone colic surgery and survived to discharge, reporting that 63-73% returned to racing. Furthermore, surgical treatment did not appear to negatively impact athletic performance. A similar finding was also seen in the general sport horse population.
Despite significant advancement in colic surgery per se, complications following surgery can have a significant impact on post-operative survival and return to athletic function. Common post-operative complications include:
Complications at the site of the incision (surgical wound)
Infection: Infections at the site of the surgical incision are relatively common. Antibiotics are usually administered before surgery and after surgery. Infections are not normally severe but can increase treatment costs. Horses that develop infections are at greater risk of developing an incisional hernia.
Hernia: Incisional hernias occur when the abdominal wall muscles fail to heal leaving a ‘gap’. Hernia size can vary from just a few centimetres, up to the full length of the incision. Most hernias will not require further treatment, but in more severe cases, further surgery may be required to repair the hernia.
Complications within the abdomen
Haemoperitoneum: A rare complication where there is blood within the abdomen from bleeding at the surgical site.
Anastomosis complications: The anastomosis site is where two opposing ends of intestine that have been opened are sutured back together again. It is important that at this site no leakage of intestinal contents occurs. Leakage or breakdown at this site can lead to peritonitis, which is inflammation or infection within the abdominal cavity and is a potentially life threatening complication.
Adhesions: Scar tissue can form within the abdomen following abdominal surgery. Occasionally this may cause further colic episodes
Further colic episodes
Further colic episodes can occur following surgery. These can occur days to months following discharge.
Endotoxaemia
In some rare cases, horses may develop sepsis in response to toxins released by damaged intestine
Diarrhoea
This is a rare complication. It can develop as a result of infections with C. difficile or Salmonella. As a consequence, some horses may need to be treated in isolation to ensure infection doesn’t spread to other horses or humans.
Post-operative ileus

Post-operative ileus is one of the potential post-operative complications which can lead to a significant increase in hospital stay duration, increased treatment costs and is also associated with reduced survival rates. Post-operative ileus is a condition that affects the muscle function in the intestinal wall. The intestine is a long tube-like structure that has a muscular wall throughout its entire length from the oesophagus to the anus. The function of this muscle is to contract in waves to mix and move food along the length of the intestinal tract, within which digestion occurs and nutrients are absorbed, terminating in the excretion of waste material as faeces. In post-operative ileus these contractions stop and thus intestinal contents are not moved throughout the intestinal tract. In most cases, it is transient and lasts for up to 48 hours following surgery; however, in some cases it can last longer. A build-up of fluid develops within the intestine as a result of the lack of propulsion. This stretches the intestines and stomach, resulting in pain and the horse’s inability to eat. Unlike humans, the horse is unable to vomit; consequently, this excess fluid must be removed from the stomach by other means, otherwise there is a risk of the stomach rupturing with fatal consequences. Post-operative ileus may occur in up to 60% of horses undergoing abdominal surgery and mortality rates as high as 86% have been reported. Horses in which the small intestine manipulated is extensively manipulated during surgery and those that require removal of segments of intestine are at higher risk. Despite the significant risk of post-operative ileus following colic surgery in horses, there is a lack of studies investigating the mechanisms underpinning this condition in horses; consequently, the precise cause of this condition in horses is not fully known.
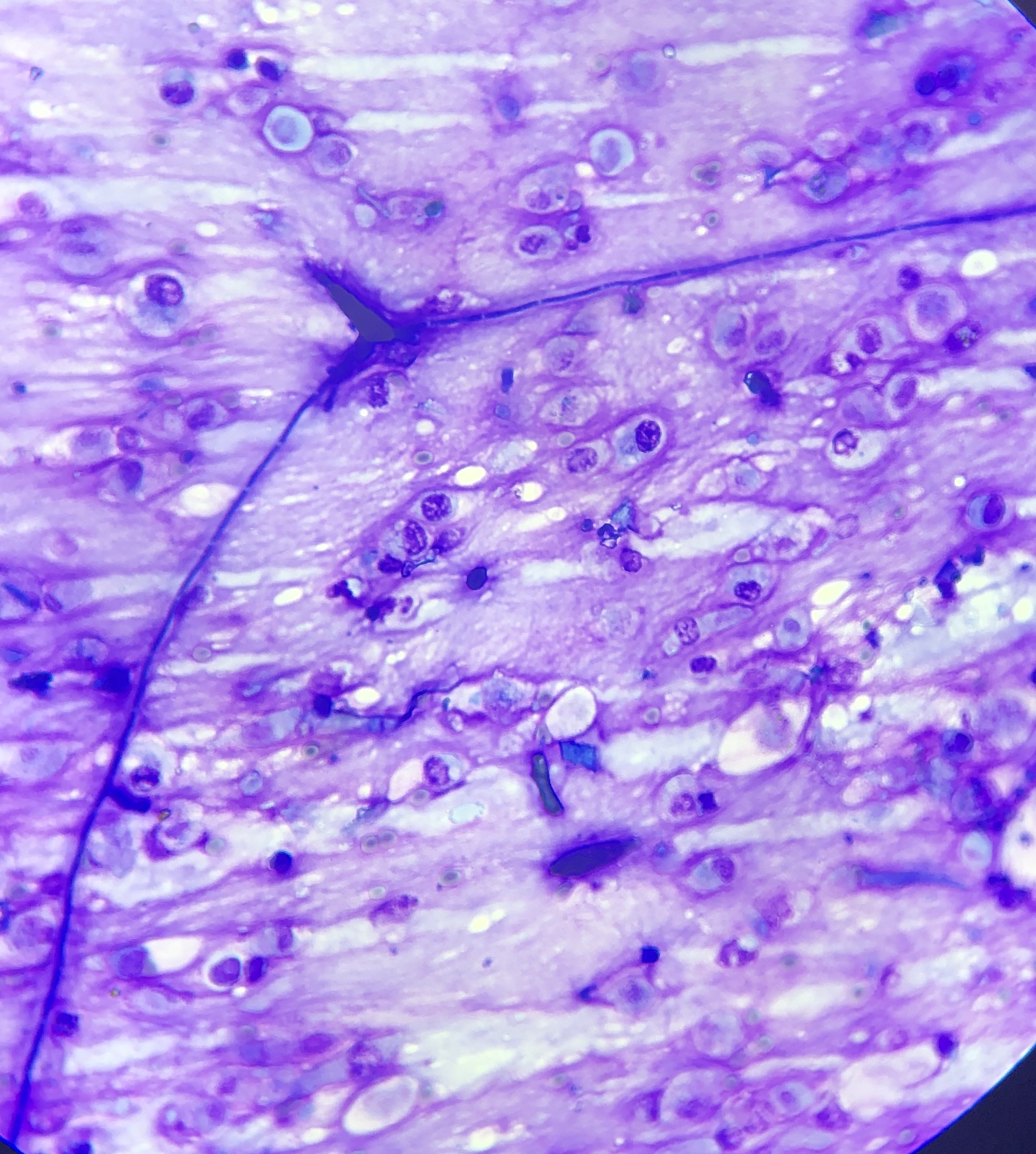
What causes the intestine to stop functioning?
For many years it was thought that post-operative ileus occurred as a result of a dysfunction of the nerves that stimulate contraction of the muscles in the intestinal wall. This theory has now mostly been superseded by the concept that it primarily results from inflammation in the intestinal wall. Based on human and rodent studies, it has been shown that immune cells in the intestine (macrophages) play a key role in development of this condition. Macrophages are important cells found everywhere in the body, with the largest population being in the intestine. These cells become activated by the inevitable manipulation of the horses’ intestines during colic surgery, with subsequent initiation of a sequence of events which ultimately results in dysfunction of the muscle in the intestinal wall. We know macrophages are present within the wall of the horses’ intestine and that at the time of colic surgery there is an inflammatory response at this site. Although the significance of these findings in relation to post-operative ileus in the horse remains unknown, they provide sufficient justification for ongoing research focused on the inflammatory response in the intestine of horses during and immediately following colic surgery…