Fungi - the invisible health risk

Dr. Emmanuelle van Erck, DVM, PhD, ECEIM explains her work looking at the link between the presence of fungi and lower airway inflammation
Horses are incredible athletes. Their physiology—the way their body functions—is truly fascinating. They can adapt to training at a phenomenal rate, they have massive hearts that fuel their powerful muscles and pushes them to peak speeds. So what could stop them? Oxygen, or rather the lack of it. Horses experience hypoxemia during racing, which means they enter a state of deficiency in oxygen. The reason for this deficiency is a failure of the respiratory system to effectively ventilate and adequately fuel oxygen to the muscles. Horses are obligate nasal breathers and were endowed with particularly long and narrow upper airways in relation to their body size. These factors increase the resistance to breathing. They are also constrained by the fact that they ventilate at very high rates, which does not allow for effective and rapid renewal of oxygen in the lungs. Even the fittest, best thoroughbreds crave oxygen from mid-race onwards. So maintaining horses in optimal respiratory health is absolutely essential for them to achieve an efficient sprint and optimal performance.
Respiratory diseases are highly prevalent in horses. It is inherent to their living and working conditions. The mere fact that a horse is housed in a box increases his risk of developing airway inflammation. The content in fine dust is naturally high in a horse’s box. Closed or poorly ventilated barns further deteriorate air quality in the horse’s immediate environment. Several studies have shown that horses housed indoors are exposed not only to high amounts of organic dust and ammonia but also germs and endotoxin they produce that trigger a detrimental reaction from the immune system. The problem is that even low-grade respiratory diseases will directly affect the horse’s capacity to perform and recover from strenuous exercise.
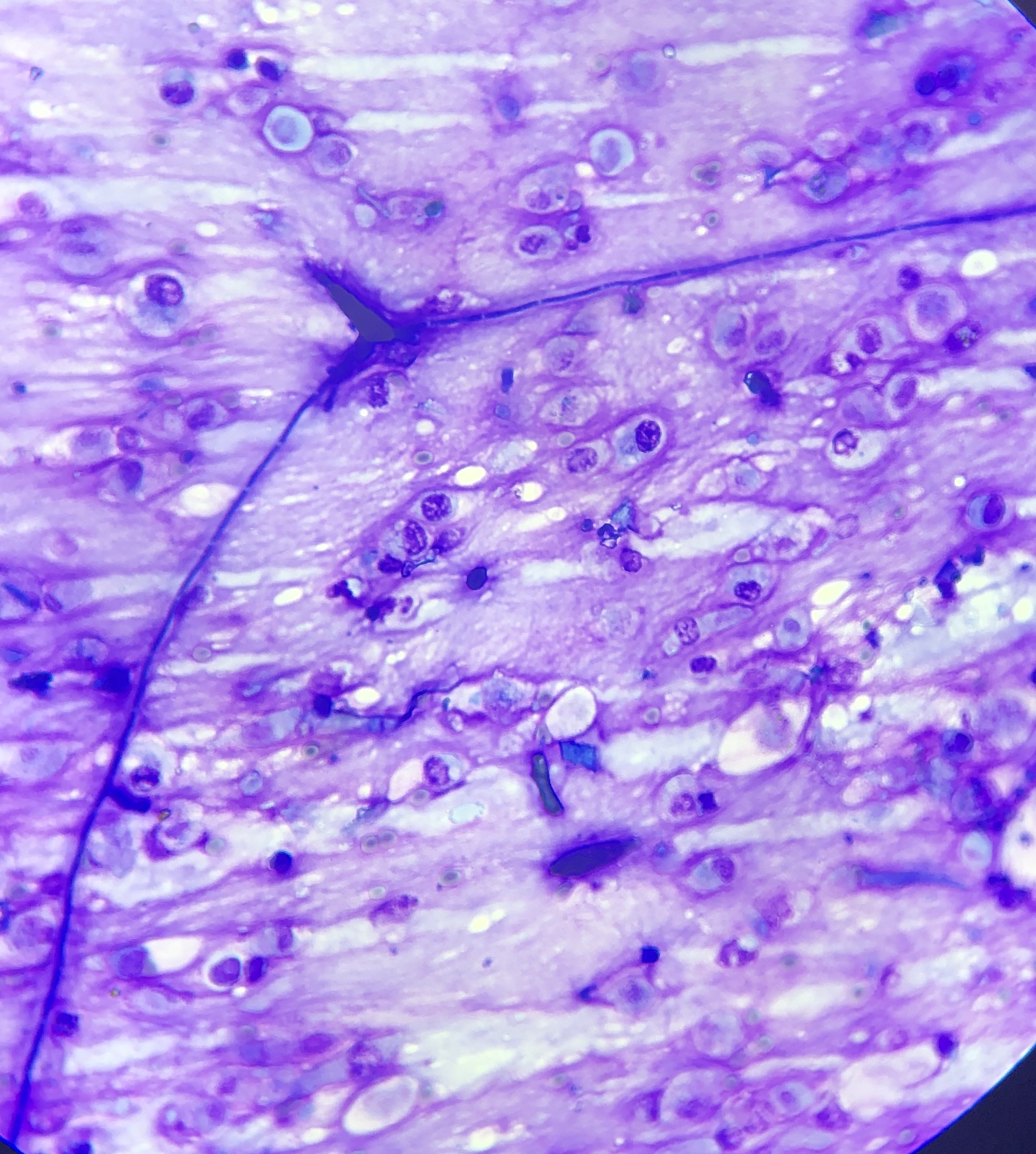
Microscope picture of a germinating fungal spore in a respiratory sample - an indication of inhalation of fungal spores in the airways and subsequent infection from the mould.
With my colleagues, Dr Dauviller and Dr ter Woort, specialists in equine internal medicine, we have investigated the link between the presence of fungi and lower airway inflammation. In our ambulatory referral practice, we go out to the stables and have the opportunity not only to examine the horse but also attentively assess his environment. As we collected respiratory samples and analysed them ourselves, we became aware that the presence of microscopic moulds or fungal elements was frequently associated to lung issues. To investigate this further, we decided to systematically record clinical and environmental data and link it to our findings in the respiratory samples of the horses referred for investigation.
We collected more than 700 cases; the horses included in the study were either referred routine examinations, unexplained poor performance or respiratory symptoms such as coughing or breathing heavily during exercise. All horses had a tracheal and a bronchoalveolar lavage done which allowed us to evaluate their level of respiratory inflammation, as well as estimate the presence of fungi within the airways. We also looked at the state of activation of fungi: if they were inert particles or if they showed signs of active proliferation. Our results were without appeal; the presence of inhaled fungi significantly and negatively affected respiratory health in horses, causing inflammation and in some cases, infection.
In this population, inflammatory airway disease (IAD) was diagnosed in 88% of cases, confirming that respiratory inflammation is very common and often under-diagnosed. Of these positive cases, 81% had evidence of fungi in their airways. The presence of fungi more than doubled the odds of having lung inflammation.
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Streptococcus zooepidemicus - The bug that can place bets
The Horserace Betting Levy Board (HBLB) has invested over £7 million to protect racing and ensure horse welfare by disease surveillance and research on prevention of equine infections over the last decade. Infection with bacteria is one of the important causes. One bug in particular that can be found in many cases is Streptococcus zooepidemicus.
Respiratory disease affects a large proportion of young horses around the world, reducing performance with significant disruption to training and racing schedules. Inflammatory airway disease affects young horses in particular and it generally causes mucus in the trachea. Some estimates suggest that in British Flat racing yards, for every 100 horses, each month there will be nine cases.

Coughing and nasal discharge can last around eight weeks and some animals are affected again and again. All of which leads to significant cost to the racing industry. As a result, this problem has been a long-standing focus of attention for the Horserace Betting Levy Board’s (HBLB) veterinary research efforts.
Bacterial genetic code
One reason why bacteria from the same species might affect horses differently is that there are different strains within a bacterial species. This is rather like different breeds of horses – a Falabella pony is the same species as a thoroughbred – but it looks and acts very differently. All living things, from human to single-cell algae in the ocean, have a genetic code written in DNA. Understanding this genetic code can reveal how organisms live and function.
“In the same way as Strangles, a horse that has recovered from Streptococcus zooepidemicatus might no longer be outwardly affected itself but it may still carry the bug”
An HBLB-funded collaborative team working in Dr Andrew Waller’s lab at the Animal Health Trust and Professor Josh Slater’s lab at the Royal Veterinary College have set out to unlock the genetic make-up of different strains of Streptococcus zooepidemicus in order to understand better if some strains of this bacteria cause disease while others are relatively harmless. The researchers also looked at how different strains of Streptococcus interact with the horses’ immune system. The ulitmate goal of this research is to gain the knowledge which will lead to new vaccines.
A global research effort
The researchers started by developing a technique to produce a unique ‘genetic fingerprint’ with which to identify each different strain of the Streptococcus. They then tested samples from sick horses around the world and so far 318 different types of S. zooepidemicus have been identified with two particular strains being responsible for outbreaks of respiratory disease.
Insight from an ancient threat: Strangles
The researchers had some clues about what they might find in the samples from horses with Streptococcus zooepidemicus infection because they already had extensive experience in similar research in Strangles. Strangles is one of the oldest known, feared and most frequently reported infectious diseases of horses throughout the world. Typical signs of Strangles include abscessation of the lymph nodes in the head and neck, with swelling to such an extent that some horses are literally suffocated. It is caused by a relative of Streptococcus zooepidemicus, known as Streptotococcus equi. With Strangles, it is very clear that some recovered horses become carriers. Carriers show no outward signs and this hidden infection enables the bacteria to be spread around undetected.

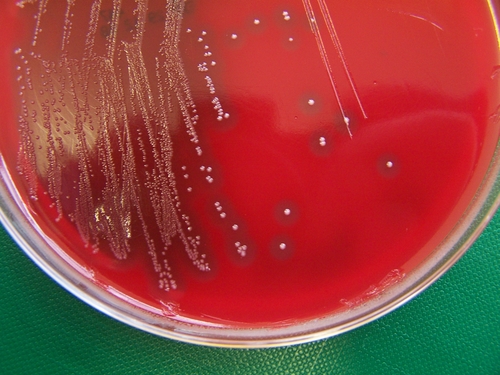
S. zooepidemicus colonies grown on a blood agar culture plate
Silent carriers lead to infection in youngsters
In the same way as Strangles, a horse that has recovered from Streptococcus zooepidemicatus might no longer be outwardly affected itself but it may still carry the bug. For example, the particular strain responsible for the outbreak of respiratory disease in Sweden was found in a healthy horse eight months after the horse made a full clinical recovery.
This persistence of S. zooepidemicus in thoroughbred racehorses that have recovered from respiratory disease allows transmission to susceptible animals and can occur when, for example, older recovered horses are mixed with the next year’s intake of young horses. It is likely that immunity to one strain of Streptococcus does not fully protect a horse from all the other strains, so young horses can often succumb to a succession of respiratory infections as they gradually build up immunity to mix of Streptococcus zooepidemicus strains that persist in that particular yard.
Bacterial balancing acts
In order to be able persist in recovered horses Streptococcus zooepidemicus must be able to survive despite the fact it is being attacked by the horse’s immune response, and at the same time, the bug must be ready to infect a susceptible animal should the opportunity arise. S. zooepidemicus strains have proteins on their surface and some of these proteins inactivate the horse’s immune response. Other proteins enable the bacteria to stick to the internal surfaces of the horse in order to establish the infection, almost like an ice climber clinging to the surface of a glacier with the crampons on his boots. If he loses his crampons, he is in big trouble.
Thus, these surface proteins play key roles for the bacteria, but they are also a vunerable point and can be targeted by the horse’s immune response to disable the bacteria. Therefore, balancing the array of surface proteins displayed with the particular requirements of the bacteria at any given time is critical if the bacteria are to successfully establish an infection and transmit to a new susceptible animal.
THERE'S MORE TO READ ONLINE....
THIS ARTICLE FIRST APPEARED IN EUROPEAN TRAINER - ISSUE 47
TO READ THIS ARTICLE IN FULL - CLICK HERE
Author: Celia Marr, Andrew S. Waller & Josh Slater
Training the untrainable - how to improve the respiratory system
Most body systems of the horse have some capacity to respond to physical training of the type used to improve fitness and performance in Thoroughbred racehorses. The art of training is of course assessing what each horse needs, when to start, when to back off and when to accept that you have reached a suitable level of fitness which should result in a horse being able to get close to achieving a performance consistent with its genetic potential. However, the one body system that training cannot improve on is the respiratory system and this article will highlight some of the implications of this.
Dr David Marlin (17 September 2008 - Issue number 9)
By David Marlin
Most body systems of the horse have some capacity to respond to physical training of the type used to improve fitness and performance in Thoroughbred racehorses. The art of training is of course assessing what each horse needs, when to start, when to back off and when to accept that you have reached a suitable level of fitness which should result in a horse being able to get close to achieving a performance consistent with its genetic potential. However, the one body system that training cannot improve on is the respiratory system and this article will highlight some of the implications of this.
So are winners born or created and how important is physical training? In my view the best racehorses are born with or without potential. Its true that a lot can go wrong from the moment a stallion and mares genes mix to produce an embryo that will grow into a foal. Often underestimated is the impact that the environment within the mare has on the development of the foal. For example, the genes may be saying “straight legs” but other factors such as stress on the mare, infections, diet, the condition of the uterus, may well modify how that message is “interpreted” leading to a foal with crooked legs. The impact of the uterine environment was perfectly demonstrated by some ground breaking studies by Professor Twink Allen at the Equine Fertility Unit in Newmarket, where he demonstrated that pony embryos transplanted into Thoroughbred mares resulted in large pony foals and that Thoroughbred embryos implanted into pony mares resulted in small Thoroughbred foals.
Once a foal is born, there is a long and potentially difficult path from birth to racing success, even with the right genes for performance. Diet, disease, trimming, shoeing and even luck all play a role. Then comes training. And here I am focussing on physical training rather than training the horse to run in company, quicken away from a group or go in stalls…what we might considered behavioural training. A recent scientific study from the University of Florida in the USA which looked at horses purchased at yearling sales in the summer for sale at 2-year-olds in training sales the following spring found that 37 out of 40 horses purchased became lame during training. Also interesting was the fact that “the frequency of new cases of lameness increased as the date of the 2-year-olds in training sales approached.”
The aim of training should be to maximise the genetic potential of a horse. How much is a horse born with and how much difference does training make? Scientifically that’s quite a difficult question to answer. My gut feeling is that training may add perhaps a quarter...so this leaves 75% of performance down to breeding or in other words, the genes. How do I come to this conclusion? Take a horse with a handicap rating of 70lbs with an average trainer and give it to an exceptional trainer, and the latter may be able to improve the horses rating by 15-20lbs. Its not uncommon to see a horse change trainers and increase by 10-20lbs, but to see a horse change trainers and go from a rating of 70 to 130lbs would be exceptional.
So I believe that elite horses are born, not created through management and training. That’s not to downgrade the role of the trainer. Training has to be very important. How many untrained horses win races? But we also know that poor training can take a horse with the potential to win the Derby and turn it into one that never even gets to race and good training could take a horse with an expected rating of 60lbs up to perhaps 80.
Hence, knowing that training can improve poor horses, ruin good horses and vice versa, there can be no doubt that training racehorses is a challenge. Too low of a training load and the horse performs below expectations. Too high and you risk injury; particularly of course musculoskeletal injury…injury to bone, cartilage, ligament, and tendons and to a lesser extent muscle. Getting it right for each horse is certainly a combination of art, science and skill.
Why is training horses such a challenge? Part of the problem is the way in which different body systems or components respond to training. With appropriate loading or “stress”, the locomotory muscles and the heart (which is of course also a muscle) have a tremendous capacity to adapt to repeated bouts of exercise…or training. However, the intensity and volume (amount) of exercise required to get these systems to adapt is high compared for example to the amount of loading required for healthy bone development. Thus there is a potential imbalance. The heart and locomotory muscles need relatively long durations of exercise at high intensities to cause them to adapt, but this amount of exercise loading is often in excess of what joints, bones and tendons need or are built to cope with.
During training, the period where there is a high risk of injury is also the period when there is the greatest need for “stress” to increase fitness and performance. Eventually there is some balance achieved between muscle fitness, performance and musculoskeletal injury – the green zone. However, there is one body system – the respiratory system - that never attains this balance and for which exercise almost appears to be contra-indicated. In fact, it may come as a surprise to many to learn that the respiratory system of the horse does not respond to training. The amount of air an unfit/untrained horse moves in and out with each breath with each stride at the walk, trot, canter and gallop does not change when that horse is fit/trained. Many refuse to accept this, but at least three independent scientific studies, including one in my own laboratory, have confirmed this.
Is the lack of adaptation of the respiratory system of the horse to training a problem? Well it is a problem when that system is a limiting factor or weak point in the chain to get oxygen from the outside down to the muscles where it can be used. In unfit/untrained racehorses the heart is probably the limiting factor to performance. But with training the heart adapts, leaving the respiratory system as the “weakest link”, even thought it is crucial to racing performance. Unless we want to race over distance of 1 furlong or less, the respiratory system is essential. Even in a 5 furlong sprint race around 70% of the energy to run comes from aerobic metabolism that requires oxygen to be brought into the body by the respiratory system, to allow the conversion of energy in sugars, stored as glycogen within the muscles cells, into energy for locomotion in the form of ATP.
How do we know the respiratory system is the weakest link? Because if we can give the horse more oxygen to breathe than the normal 21% that is in air, say we increase it from 21% to 30%, we know the heart is able to transport this extra oxygen to the muscles. The muscles are able to use this extra oxygen and as a result performance is improved. (I think at this stage we can of course dismiss oxygen cylinders carried by the jockey with a tube running to the horses nostrils.) Thus, the limiting point in the chain from nostril to muscle is in the respiratory system and to be more precise, in the deeper parts of the lung where the air containing oxygen passes into the lungs and is separated from the red blood cells in blood vessels on the other side.
We also know how fragile and delicate the respiratory system of the horse is. This is usually not apparent from the outside, but only when we consider the microscopic structure of the lung. The horse’s windpipe (trachea) is around 5-8cm in diameter, but as the windpipe passes deeper in the lung it begins to divide to produce smaller and smaller airways, much like a tree on its side, with the main trunk representing the windpipe. Each time an airway divides in two, the “daughter” airways are smaller than the “parent” from which they arose. When we get down to the level of the smallest airways, after perhaps 25 divisions, the airways are fractions of a millimetre in size. When the air gets to this point in the chain from nostril to muscle cell, it has to cross from the air space into the blood vessel. This is a passive process. There is nothing that can be done to speed it up as it depends on some fixed factors such as the total surface area available in the lung for oxygen to diffuse (move) across, which does not increase with training. (Incidentally, the total area for oxygen to diffuse across in the horse is equivalent to the area of 10 tennis courts!). It is also dependant on the difference in oxygen level between the air (high) and the blood vessels (lower). Oxygen moves from high to low areas. Finally, it depends on the thickness of the membrane separating the air in the air sacs (“alveoli”) and red blood cells in the blood vessels (“capillaries”). So one option is to evolve to make this membrane, sometimes referred to as the blood gas barrier, as thin as possible. And this is exactly what has happened in the Thoroughbred to the point where this membrane separating blood under pressure in vessels from the air in the airways is around 1/100th of the thickness of a human hair. Perhaps not surprisingly, these small membranes can rupture under the stress of exercise allowing the red bloods cells (RBCs) to spill from the capillaries into the alveoli, which we term exercise-induced pulmonary haemorrhage (EIPH).
So if the respiratory system does not adapt positively with training, the next best thing we can hope for is that it is not damaged by training. Unfortunately, this is not the case either. Studies from Japan demonstrated that Thoroughbred racehorses that were only trained at the walk, trot and slow canter still experienced rupture of small blood vessels in the lung. It is also true that the harder and more frequently a horse works, the greater the number of vessels that will rupture and therefore that this damage is cumulative. There is individual variation of course, with some horses being minimally affected and some horses affected to the extent that they are effectively untrainable. And to dispel a myth; this damage (EIPH) is occurring even if you do not see blood at the nostrils or even in the trachea (with a ‘scope) after exercise.
What are the consequences of the rupture of these small vessels? Perhaps the best analogy is to drinking. The bad news is that a bottle of wine may kill off 10 million brain cells. The good news is we start with around 100 billion brain cells. However, after 10 years of heavy drinking the effects can begin to show! In this respect, the lungs are no different, however, the effects are noticeable much sooner.
How many small blood vessels are there in the lung? Its hard to be precise about this, but if we work on the fact that there are 40 generations of airways (divisions or branches) in the horses lung and if each small airway had a small blood vessel around it, then this would give a figure of around 270 billion. How many break at Canter? At Gallop? In a race? Impossible to estimate and again it varies between horses. But what we do know is that after time we can see scarring on the lung surface as a result of previous injury (haemorrhage).
Contrast the relatively undamaged and unstained lungs of an untrained horse on the left with those on the right. Note the deep blue/grey staining showing areas of previous damage on the right, accumulated over many years of training and racing. Blood vessels that are damaged do not regenerate. Scar tissue forms and these areas cease to function normally. The more damage that accumulates, the greater the reduction in respiratory function.
One question that has always intrigued me is how much damage to the lung occurs as a result of broken blood vessels (EIPH) in racing relative to how much occurs in training? One way to try and work this out would be to give a “damage score” to different types of activity and then total up. For example, we could arbitrarily assign a value of 1 (i.e. low) for the damage caused by a slow canter and 3 for a fast canter….i.e. causing more damage. If we then scored a fast canter as 5 and a piece of work at home as 10, then we might put a value of 40 on the damage to the lung caused by a single race. Assuming 6 exercise days per week and therefore 24 exercise days a month from January to October, and starting with 48 days of slow canter in Jan-Feb, 36 days medium canter in Feb-Mar, etc, over this period our horse would have 48 bouts of slow canter, 108 bouts of medium canter, 108 bouts of fast canter and 52 pieces of work.
I’m then going to assume our horse ran 5 times in this 10 month period. When we total up the damage caused by training and compare it to that caused by racing, we may get a surprise. Although the damage in racing is more severe, the races are much less frequent and the total estimated damage by racing is only 12% of the total in this example. This leaves 88% of the damage to the lungs occurring during training – less damage per training day, but more training days. This type of approach shows us that perhaps it’s training, rather than racing, that we need to be more concerned about as far as EIPH.
So if significant damage is occurring to the lungs as a result of training and racing, what options are there in management? There seem to be an ever increasing number of products marketed for bleeders. However, there are only two treatments that have been scientifically proven to significantly reduce bleeding in horses; Lasix and nasal strips.
Lasix and nasal strips actually both work in a similar way in reducing stress on the blood vessel walls. Lasix works by decreasing the blood pressure in the blood vessels inside the lung and hence decreasing the stress on the walls and reducing the number that rupture. Nasal strips also work by reducing the stress on the wall of the blood vessel walls, but from the air side.
Lasix is a type of drug known as a diuretic. When given to horses it “tricks” the kidneys into producing more urine than normal. This in turn removes water from the blood, reducing the volume of plasma (the watery part of the blood as opposed to the red blood cells) in the circulation. This reduces the blood pressure so that the tiny blood vessels in the lung are less stretched and stressed.
The nasal strip works on the other side of these blood vessels in the lung – the side that is in contact with the air. Nasal strips work by supporting the loose flap of skin behind each nostril. When the horse breathes in this skin is sucked inwards. The more this skin is sucked in the more effort the horse needs to make to move air into the lungs. Horses, unlike us, only breathe through their nostrils, and so any obstruction in this area can have a big effect. This effort in breathing in causes the walls of the tiny blood vessels (known as capillaries) to bulge outwards and in some cases break, resulting in the loss of blood into the air spaces and tubes of the lung. The nasal strip supports this skin over the nose and allows the horse to move the same amount of air in and out with less effort, placing less stress on the lung.
So two treatments. In scientific trials, they showed the same level of effectiveness in reducing bleeding. One is a drug and one is mechanical. Does it matter which one you use? On a one off gallop probably not. However, with repeated use of drugs tolerance often develops. This may mean that over time you have to use larger and larger doses to get the same effect. Or alternatively, if you keep using the same dose then the effect you get becomes less and less. It is also not uncommon for drugs to have unwanted side effects with repeated use. The degree of dehydration induced by Lasix is also something to consider. Dehydration can have adverse effects on many systems, for example the digestive tract. Whilst to date no-one has looked at the effects of the dehydration resulting from use of Lasix alone on body systems other than the lung, trainers and veterinarians need to be careful to consider other possible factors that will increase dehydration further, such as hot weather, transport and sweating and decreased water and feed intake due to anxiety. The potential advantage of a mechanical device, such as the nasal strip, for treatment of bleeding is that it is almost certainly going to be equally effective each time it is used, tolerance is highly unlikely and there is no possibility of any side effects.
On the basis that each treatment works, is their any advantage to using both? The answer appears to be yes based on a study of horses racing in the USA. Even though both Lasix and nasal strips work on the blood vessel wall, severe bleeders still showed a further reduction in bleeding of 65% when they raced with a nasal strip and were treated with Lasix, compared to being treated with Lasix alone.
On paper, if you listed out the potential problems in training an animal where what one body system needs is what might break another body system, you would have to conclude that training horses is going to be extremely challenging. This is perhaps testament to the high level of skill that any moderately successful trainer clearly must have developed. Training clearly cannot be approached as a pure science and in fact there are some examples of very good scientists who have made poor trainers. But science can potentially help trainers understand more about how the different body systems of the horse respond to training and apply their skills more effectively.
Nasal Strips - increasing performance, reducing EIPH
Nasal strips’ future in Thoroughbred racing seemed limitless in the fall of 1999. Just two weeks after longshot Burrito won a race at Keeneland wearing one, 29 of the 101 horses competing in the 1999 Breeders’ Cup at Gulfstream Park November 6th had the 4-by-6-inch strip affixed 1.5 inches above their nostrils.
Bill Heller (European Trainer - issue 18 - Summer 2007)
Nasal strips’ future in Thoroughbred racing seemed limitless in the fall of 1999. Just two weeks after longshot Burrito won a race at Keeneland wearing one, 29 of the 101 horses competing in the 1999 Breeders’ Cup at Gulfstream Park November 6th had the 4-by-6-inch strip affixed 1.5 inches above their nostrils. More importantly, three of the eight winners wore them, including Cat Thief, who captured the $4 million Classic at odds of 19-1 under Pat Day, who was sporting a human equivalent, himself. The image of both Cat Thief and Day posing in the winner’s circle with nasal strips was a powerful one. Cat Thief’s victory was the second that day for Hall of Fame trainer D. Wayne Lukas, who earlier saddled 32-1 longshot Cash Run to win the $1 million Breeder’s Cup Two-Year-Old Juvenile Fillies.
She, too, wore the non-invasive strip designed to reduce an exercising horse’s airway resistance and decrease exercise-induced, pulmonary hemorrhaging (EIPH). The nasal strips received enormous national publicity after the Breeders’ Cup. Wouldn’t almost everyone in North America emulate Lukas? Stan Bergstein, the executive vice-president of Harness Tracks of America and a columnist for the Daily Racing Form, postulated long ago that if a horse wearing a blue balloon tied to his tail won a race, you’d see dozens of horses with blue balloons tied to their tails in the paddock the next day. Lukas, however, preached caution regarding the role of nasal strips in Cash Run and Cat Thief’s surprise Breeders’ Cup victories.
Regardless, Lukas and trainer Bob Baffert spoke at a meeting of the California Horse Racing Board Medication Committee meeting, January 12th, 2000, in support of nasal strips. According to a CHRB press release, CHRB Commissioner Marie Moretti expressed hope that using the strips could lead to the decreased use of bleeder medication for some racehorses. That never happened, as Lukas proved prophetic. He saddled three horses in the 2000 Kentucky Derby, two with nasal strips, and none of them finished higher than 12th.
According to Equibase, between October 23rd, 1999, and April 24th, 2000, 8,402 Thoroughbreds wore the strip and 1,077 won, nearly 13 percent. Apparently that wasn’t high enough. Less and less trainers used them, though Lukas still does. By the end of 2000, there was a story on the Internet site www.suite101.com entitled “The Demise of Nasal Strips.” Published December 12th, 2000, the article began, “The rise and fall of nasal strips was short and sweet.” Noting that the Daily Racing Form had originally listed the nasal strip in past performance lines for all tracks and that by mid-June was only listing them at Hollywood Park, the story concluded, “As quick as they appeared in the spotlight, they vanished.” The obituary was more than a bit premature. Miesque’s Approval won the 2006 Breeders’ Cup Mile at Churchill Downs wearing a nasal strip for trainer Marty Wolfson, who uses them on all of his 30 horses. “I’ve been using them on all my horses for two years,” Wolfson said in mid-March. “I use them on myself. I run and they help me when I run. I breathe easier. The only time I couldn’t use one was when Pomeroy was in the 2006 Forego Handicap at Saratoga.” Pomeroy won that stakes. He was denied the nasal strip at Saratoga because the New York Racing Association mysteriously banned nasal strips, a day after the New York State Racing and Wagering Board approved them for both Thoroughbred and harness racing. Currently, New Jersey is the only other state which doesn’t allow them, while Pennsylvania allows them for Thoroughbreds but not for Standardbreds. According to nasal strip co-inventor and president of Flair Nasal Strips Jim Chiapetta, some 15,000 nasal strips are sold world-wide each year: 9,000 in the United States, 3,500 in Europe, 2,000 in Australia and New Zealand and 500 in Dubai. He said they were used mostly on horses in eventing, then on Thoroughbreds, Standardbreds and Quarter Horses. Should they be used more often? Are they a realistic alternative to the powerful diuretic Lasix, which is now used by roughly 95 percent of all
Thoroughbreds in the U.S., though the rest of the horse racing world bans Lasix and all other race-day medications? Lasix, which is used ostensibly to reduce EIPH, can improve a horse’s performance dramatically the first and/or second time it is used, if for no other reason that its diuretic properties. Horses can lose 10 to 20 pounds through urination after Lasix is injected. That alone improves most horses’ performance. Think about it. If there is an apprentice jockey with even a modicum of ability, trainers scramble for his services just to decrease the weight his horse is carrying by five pounds. The efficacy of nasal strips can be judged in comparison to Lasix or by itself. “Lasix and nasal strips work in very similar ways,” said David Marlin, a consultant who worked for the Animal Health Trust in Newmarket, England, and co-authored Equine Exercise
Physiology. “From scientific studies, they seem to be equally effective in reducing bleeding.” Breathe Right strips were invented in 1987 by Bruce Johnson, who suffered from allergies. By the early 1990’s, they were being used for colds, allergies, snoring and athletic performance. They work by reducing the partial collapse of the soft tissues of the nose when it is under pressure because of the vacuum caused by the lungs during exercise. The mechanical, spring device maintains optimum air flow. Humans have an option for breathing: nose or mouth. Horses do not. They breathe only through their nostrils. Could nasal strips benefit horses? That’s a question Jim Chiapetta and his partner Ed Blach decided to explore. They had become friends at the Littleton Large Animal Clinic in Littleton, Colorado. Chiapetta, 48, returned to his clinic in Shakopee, Minnesota, to finish law school at William Mitchell College of Law. Blach, a former veterinarian who is now an animal products consultant, called Chiapetta in 1996 to discuss a possible equine version of a nasal strip. “We talked to a bunch of people and they said it wouldn’t work for horses, but I told Ed I think it could,” Chiapetta said. “We went ahead and made some prototypes.” Then they consulted Monty Roberts, the horse whisperer. “Ed used to be Monty’s resident veterinarian,” Chiapetta explained. Roberts was interested enough to have them test the strip at a track at Roberts’ farm north of Santa Barbara in California. “We didn’t have the adhesive done right,” Chiapetta said. “The riders were coming back and saying, `This horse felt better, more relaxed.’ So we figured there was something there.” Having breakfast one morning with Roberts, Chiapetta and Bloch came up with a name. “I was thinking about flaring nostrils, then I was thinking about air, and we came up with the name Flair,” Chiapetta said. Next, they consulted with CNS, the Minnesota company which manufactured Breathe Right. “They agreed to license it if it showed it reduces bleeding,” Chiapetta said. “They funded a study at Kansas State University.” That study and a majority, but not all, of a handful of subsequent studies - all involving a standard small sample of horses - showed positive results from nasal strips. “The nasal strips seem to help,” Dr. Howard Erickson of Kansas State University, a co-author of one of the studies, said last February. “We’ve done studies here.
There have been studies in Kentucky, California and Florida. In most of the studies, it decreases the bleeding by 50 percent and it also decreases the airway resistance.” He believes that most horses would benefit from both, because he believes almost all horses suffer from EIPH: “I think it’s nearly 100 percent that have some degree of bleeding for the movement of fluid from the capillaries to the airway. For some, it may be negligible. Quarter Horses will respond the same way. Standardbreds, too. You see it in rodeo horses and barrel horses.” That sentiment is shared by David Marlin, who has worked with researchers at Kansas State. “The bottom line is that all horses will break blood vessels in a race,” he said. “It happens with camels; it happens with humans, it happens with greyhounds.” Marlin also believes that nasal strips may be a more preferable treatment than Lasix. “It’s less complicated and you can’t build up tolerance,” he said. “If you think about a diabetic who uses insulin, he develops tolerance and needs more of it.
Do horses develop tolerance of Lasix? Generally, when you use drugs repeatedly, there’s a chance of adaptation to it. The nasal strip is different because it’s a mechanical device.” Then why aren’t trainers around the world, and especially in the United States, using them? Ironically, Chiapetta believes that the success of Cash Run and Cat Thief in the 1999 Breeders’ Cup is a major reason why. “It was the worst possible thing that could have happened,” he said. “We were on the front page of the New York Times Sports Section, the Wall Street Journal and Sports Illustrated. I think horsemen said, `Hey, this will make us win.’ So they strapped them on. And when they didn’t win, they took them off.” Some, not all. “They’re expensive ($7.95 per strip),” Wolfson said. “Some people don’t want to spend the money, but I think it’s worth it.” Day, the retired Hall of Fame jockey, knew they worked on him. “I found them to be quite helpful when I was riding a number of races back to back,” he said. “It seemed that I was less fatigued because I believed I was getting much more air into my lungs. I would have thought that would be more helpful to horses than riders. Horses only breathe through their noses. They cannot or will not breathe through their mouths.
If you can open up the nasal passages, open the airways, you would think it would be beneficial to the horses.” At the Havemeyer Foundation Workshop investigating EIPH, March 9th-12th, 2006, in Vancouver, Canada, Dr. Frederick Derksen, of the Department of Large Animal Clinical Sciences at Michigan State University, spoke about the role of airways in EIPH. He said, “A series of studies demonstrated that the use of a nasal strip decreases the number of red cells in bronchoalveolar laverage fluid after exercise. In horses, the majority of inspiratory resistance to airflow is located in the upper airway. The nasal valge region, located just cranial to the nasoincisive notch is a high resistance region, not supported by bone or cartilage.
These characteristics make this region particularly susceptible to collapse during inhalation. Application of the nasal strip in this region prevents nasal collapse and decreases upper airway resistance during exercise. This in turn is expected to reduce negative alveolar pressure during inhalation and decrease transmural capillary pressures.” The nasal strips are certainly a hit in New Zealand, especially with harness horses. After reading about the use of nasal strips in the 1999 Breeders’ Cup, Brian McMath, a committee member of the New Zealand Standardbred Breeders Association, imported a few samples. After the strips were approved by Harness Racing New Zealand, several trainers began using them and many had success, including Jim and Susan Wakefield’s Glacier Bay, who won the $105,000 PGG Sales Series Final at Alexandria Park in April, 2000, for trainer Cran Daigety. Eventually, Thoroughbred trainers began using the strip, too.
By the end of 2004, more than 700 winners in both harness and Thoroughbred racing won wearing the strip. “I have a technology background in chemistry and engineering, and what convinced me the strips work was basic physics,” McMath said. “It’s all about windpipe pressures and how a simple mechanical device like the springs in the nasal strip can beneficially alter these pressures.” The reception in Europe, at least for Thoroughbreds, was decidedly cooler. In an April 11th, 2000, letter, Peter Webbon, the Chief Veterinary Adviser to the British Jockey Club, noted that the senior veterinary surgeons from the European Horserace Scientific Liaison Committee (Britain, France, Italy, Germany) considered the question of nasal strips and decided to recommend to their racing authorities that their use should be banned for the following reasons: 1 “Other `gadgets’, such as tongue ties, which are allowed, are intended to address a specific clinical entity. Nasal strips are seen by trainers as a non-specific way of improving performances. 2 “If they improve performance, they should be banned, in line with performance enhancing medication. 3 “If they are ineffective, they should be banned because they give the impression that we condone practices that are intended to improve performance. 4 The manufacturers claim that they reduce the frequency/severity of EIPH.
The EHSLC veterinarians felt very strongly, for the sake of the breed, that horses should run on their merits. What would be the effect on the Thoroughbred in the long term if a horse won the Derby, wearing a nasal strip,that without the strip was unable to win a selling race?” To this day, they are banned throughout Europe for racing but allowed for training. Two years ago, Chiapetta met with Webbon and his assistant in Newmarket. “He said, `It reduces fatigue, which improves performance,’” Chiapetta related. “I said, `If you shoe them, do they run better? If you feed them, do they run better? If you train them, do they perform better? Where do you draw the line?’” Event horses are allowed to use them throughout the world because they were approved by the International Federation for Equine Sports (FEI).
On June 26th, 2006, Horse & Hound wrote that nasal strips “are becoming commonplace on the noses of top event horses,” and noted that Andrew Hoy’s Moon Fleet won the Badminton, a premier cross-country event in England. “I started using them two years ago,” Andrew Hoy said. “I’d seen them being used on horses and humans, and discussed their use with a vet. I had used a human one myself when I had a cold, and it seemed to help. I now use them on my horses at top events to give them every opportunity.” The story said that another eventer, Francis Whittington, uses them on his “advanced” horse Spin Doctor. “I tried the human version and noted the difference,” he said. “I believe it makes it easier for him to breathe so he can last the distance.” That’s the whole point. “Some people may think that more oxygen makes them run faster,” co-inventor Blach said. “That’s not the case. Rather, horses perform at their optimum level for a longer time so they can do what they’re made to do over the long haul. Maybe it’s too simple. It’s based on very simple physics that if you maintain the size of an opening, you’re going to maximize what goes through it, in this case air.” Asked if nasal strips help horses, Blach said, “Absolutely.” Perhaps the most confounding question about nasal strips is that even the single negative clinical study about them said that they do not reduce EIPH, but offered no tangible downside to their usage. Asked if there is a downside, Marlin said, “I think, as far as anyone knows from a scientific point of view, there is no evidence that there is.” Referring to that study, Chiapetta said it showed that horses using them “certainly weren’t less healthier. I don’t think there’s any downside to it.” Dr. Ted Hill, the New York Racing Association steward for the Jockey Club, said on April 11th, “Our only downside was how to regulate it. If a horse comes to the paddock and it falls off, what do we do? Do we treat it as equipment? We can’t put it back on. The significant problem we had originally was it possibly being an aid to bleeders, and relaying that to the public. That came up in an international meeting at a round table in Tokyo last October. It did not receive wide acceptance because it has some efficacy.”
So Japan does not allow them. Australia allows them for Standardbreds, but not for thoroughbreds. Yet, nasal strips are allowed for Thoroughbreds in Dubai and Singapore, as well as New Zealand. “It’s probably been embraced more in other countries than here, but in Thoroughbred racing here, furosemide (Lasix) is so embedded,” Kansas State’s Erickson said. “Furosemide reduces weight. It certainly reduces bleeding. But maybe we have to look for something better.” Maybe something better has been out there for eight years.
Inhalation therapy - treating airway problems in the racehorse
Physiologically speaking, one of the major limiting factors to racehorse performance is how efficiently the lungs can exchange gasses. Clearly any threat to the efficiency of the lungs will result in poor performance.
Paul Peacock (European Trainer - issue 14 - Summer 2006)
Physiologically speaking, one of the major limiting factors to racehorse performance is how efficiently the lungs can exchange gasses. Training maximises the potential of any athlete, equine or human, to continue functioning at full throttle while the metabolism changes to deal with an oxygen debt in the muscle tissues. Clearly any threat to the efficiency of the lungs will result in poor performance. Horses are subject to a wide range of respiratory diseases; heaves, lung bleeding or exercise- induced pulmonary haemorrhage (EIPH), and exercise induced Airway Inflammatory Disease (IAD) among them. Another description of the same basic problem is Chronic Obstructive Pulmonary Disease or (COPD). Like all mammals, horses suffer from allergic reactions as well as viral and bacterial infections. The epithelial linings of the airways and the lungs are sensitive to infection or foreign bodies of any size, and the result is usually a mucosal discharge which blocks the airway.
Whichever route an animal has airway problems, by infection or allergy, the result is almost the same; mucous builds up, coughing and irritation, frequent nose bleeding and considerably reduced performance. Moreover, some animals with tendencies towards heaves can show little signs of respiratory stress at times, but can be triggered later, more frequently by pollen and dust, when a change in regime occurs. The treatment options can be quite different for horses with a zootic infection to those with an allergy. Treatment of IAD involves the use of bronchial dilators and steroids, which have treatment implications of their own. Some of the drugs used can cause the gut to become sluggish, and can lead to colic.
Many of them induce tachycardia, the speeding of the heart rate, and still others make the animal skittish and nervous. Similarly, the use of corticosteroids in cases of allergic response, can affect the immune system, lead to numbers of other opportunistic infections, particularly in the mouth and have been implicated in laminitis. Bronchodilators include substances well known to human medicine and their function is to cause the dilation of the airways, thus allowing more air in and out of the lung. When irritated, the airways constrict and then produce mucous, which is then countered by the drug. There are two types of drug used for dilation of the airways, and they work very differently in the horse.
The Salbutamol type inhalation works on receptors on the epithelial cells of the airway, relaxing the muscle, thus causing dilation. They work at best for around an hour. A second class of drug, anticholinergics, work on various parts of the larger airway. Consequently, a mixture of the two types of drug is frequently used. Nigel Haizelden of the Ledston Equine Clinic in Castleford, West Yorkshire has been using this therapy for over 12 years and states that all kinds of drugs are administered using this system. Using a nebuliser, antibiotics, corticosteroids and bronchodilators are regularly applied. He points out that “the nebuliser is used to get the specific particle size which is required to reach a certain part of the lung – this is critical to the treatment.” Another important aspect of the bronchodilator is that the easier breathing allows the animal to relax under exercise, something which tends to promote further airway dilation. However, they do nothing for inflammation. Treatment should be associated with a regime which removes the animal from possible irritants. Trainer magazine has dealt with varying aspects in recent issues, from dust-free bedding to pollen allergy; particularly that produced by Oil Seed Rape.
One of the problems of treatment has included the fact that in order to get the drugs into the animal, the whole horse has to be treated. Injecting a horse with drugs means providing a high enough concentration in the animal’s blood which, when diluted by the circulatory system and metabolised by the liver, there is enough at the site of operation to do its work. Consequently a much higher concentration of drug is used than would be required if it could somehow be administered solely where it is needed and nowhere else. Inhalation therapy has been used in humans for a long time, from the vapour baths of Victorian days to modern viral carrier gene manipulation therapy proposed for such disorders as cystic fibrosis.
There are a number of benefits. Firstly the lung is an excellent way of getting a balanced concentration of drug into the blood stream. It works very quickly. In the case of airway disease, the drug is being used directly at the point that it is needed, and consequently the amount of drug required to be effective is greatly reduced. This improves treatment options by reducing the possibility of side effects. There are a couple of products on the market that allow this type of therapy. The Aeromask and the Equine-haler. Both are available via the vet and come from the United States. Their use has become increasingly widespread across Europe, particularly in France and Germany, where there have been particular links with American racing practices. IN the UK they have been used for at least fifteen years and the treatment regimes have developed accordingly. The Aeromask is strapped onto the head and the drug is held in a reservoir called the spacer. The Equine-haler is a cone which has to be held over the nose of the animal while the drugs are placed in a compartment at the bottom. This allows for a metered dose aerosol to deliver a dose to the spacer which is then inhaled by the horse. It only works on one nostril, and a puff of medicine is released into the nose.
The Equine-haler need not be held in position all the time, it allows for a puff of medicine to be fired into a spacer which then can be applied to the horse when it breathes in next time. Between the two it should be possible to find a regime which will ideally suit any animal, those shy of the head bag of the Aeromask could easily treated by the Equine-haler and visa versa according to the treatment required. It is important that only a measured amount of drug is administered, under veterinary control, so that overdoses do not occur. Similarly, the equipment should not be used to administer anything other than prescribed medicines. One yard on the continent was reported to have used their own remedies in association with the mask, which consequently caused some blistering to the horse’s mouth.
There are some risks associated with the use of inhalation therapy. One is associated with the drugs themselves. These drugs are particularly effective on the metabolism of the animal. It produces dilation of blood vessels, particularly in the liver, and it also promotes the production of insulin. In America at least, where there are different rules in various states regards doping, trainers are advised to take advice before racing. However, this method of treatment has meant that withdrawal periods for horses under treatment are considerably reduced in comparison to former treatments. Another possible problem is associated with the effect of the drug on the mouth, where fungal infections have been associated in humans with constant use.