Air Quality and Air Pollution’s Impact on Your Horse’s Lungs
There’s nothing like hearing a horse cough to set people scurrying around the barn to identify the culprit. After all, that cough could mean choke, or a respiratory virus has found its way into the barn. It could also indicate equine asthma. Yes, even those “everyday coughs” that we sometimes dismiss as "summer cough" or "hay cough" are a wake-up call to the potential for severe equine asthma.
Formerly known as heaves, broken wind, emphysema, chronic obstructive pulmonary disease (COPD), or recurrent airway obstruction (RAO), this respiratory condition is now called severe equine asthma (sEA). These names reflect how our scientific and medical understanding of this debilitating disease has changed over the years. We now consider heaves to be most comparable to severe asthma in people.
But what if your horse only coughs during or after exercise? This type of cough can mean that they have upper airway irritation (think throat and windpipe) or lower airway inflammation (think lungs) meaning inflammatory airway disease (IAD), which is now known as mild-to-moderate equine asthma (mEA). This airway disease is similar to childhood asthma, meaning that it can go away on its own. However, it is still very important to call your veterinarian out to diagnose mEA. This disease causes reduced athletic performance, and there are different subtypes of mEA that benefit from specific medical therapies. In some cases, mEA progresses to sEA.

Equine Asthma and Air Quality
What does equine asthma have to do with air quality? A lot, it turns out. Poor air quality, or air pollution, includes the barn dusts—the allergens and moulds in hay and the ground-up bacteria in manure, as well as arena dusts and ammonia from urine. Also, very importantly for both people and horses, air pollution can be from gas and diesel-powered equipment. This includes equipment being driven through the barn, the truck left idling by a stall window, or the smog from even a small city that drifts nearly invisibly over the surrounding farmland. Recently, forest-fire smoke has been another serious contributor to air pollution.
Smog causes the lung inflammation associated with mEA. Therefore, it is also likely that air pollution from engines and forest fires will also trigger asthma attacks in horses with sEA. Smog and smoke contain many harmful particulates and gases, but very importantly they also contain fine particulate matter known as PM2.5. The 2.5 refers to the diameter of the particle being 2.5 microns. That’s roughly 30 times smaller than the diameter of a human hair. Because it is so small, this fine particulate is inhaled deeply into the lungs where it crosses over into the bloodstream. So, not only does PM2.5 cause lung disease, but it also causes inflammation elsewhere in the body including the heart. Worldwide, even short-term exposure is associated with an increased risk of premature death from heart disease, stroke, and lung cancer. This PM2.5 stuff is not trivial!
In horses, we know that PM2.5 causes mEA, so it’s logical that smog and forest-fire smoke exposure could exacerbate asthma in horses, but we don’t know about heart disease or risk of premature death.
Symptoms, Diagnostic Tests and Treatments

Equine asthma manifests with a spectrum of symptoms that vary in severity and the degree of debilitation they cause. Just like in people with asthma, the airways of horses with mEA and sEA are “hyperreactive.” This means that the asthmatic horse’s airways are extra sensitive to barn dusts that another horse’s lungs would just “ignore.” The asthmatic horse’s airways constrict, or become narrower, in response to these dusts. This narrowing makes it harder to get air in and out of the lungs. Think about drinking through a straw. You can drink faster with a wider straw than a skinnier one. It’s the same with air and the airways. In horses with mEA, the narrowing is mild. In horses with sEA, the constriction is extreme and is the reason why they develop the “heaves line”; they have to use their abdominal muscles to help squeeze their lungs to force the air back out of their narrow airways. They also develop flaring of their nostrils at rest to make their upper airway wider to get more air in. Horses with mEA do not develop a heaves line, but the airway narrowing and inflammation do cause reduced athletic ability.
The major signs of mEA are coughing during or just after exercise that has been going on for at least a month and decreased athletic performance. In some cases, there may also be white or watery nasal discharge particularly after exercise. Often, the signs of mEA are subtle and require a very astute owner, trainer, groom, or rider to recognise them.
Another very obvious feature of horses with sEA is their persistent hacking cough, which worsens in dusty conditions. “Hello dusty hay, arena, and track!” The cough develops because of airway hyperreactivity and because of inflammation and excess mucus in the airways. Mucus is the normal response of the lung to the presence of inhaled tiny particles or other irritants. Mucus traps these noxious substances so they can be coughed out, which protects the lung. But if an asthma-prone horse is constantly exposed to a dusty environment, it leads to chronic inflammation and mucus accumulation, and the development or worsening of asthma along with that characteristic cough.
Accurately Diagnosing Equine Asthma

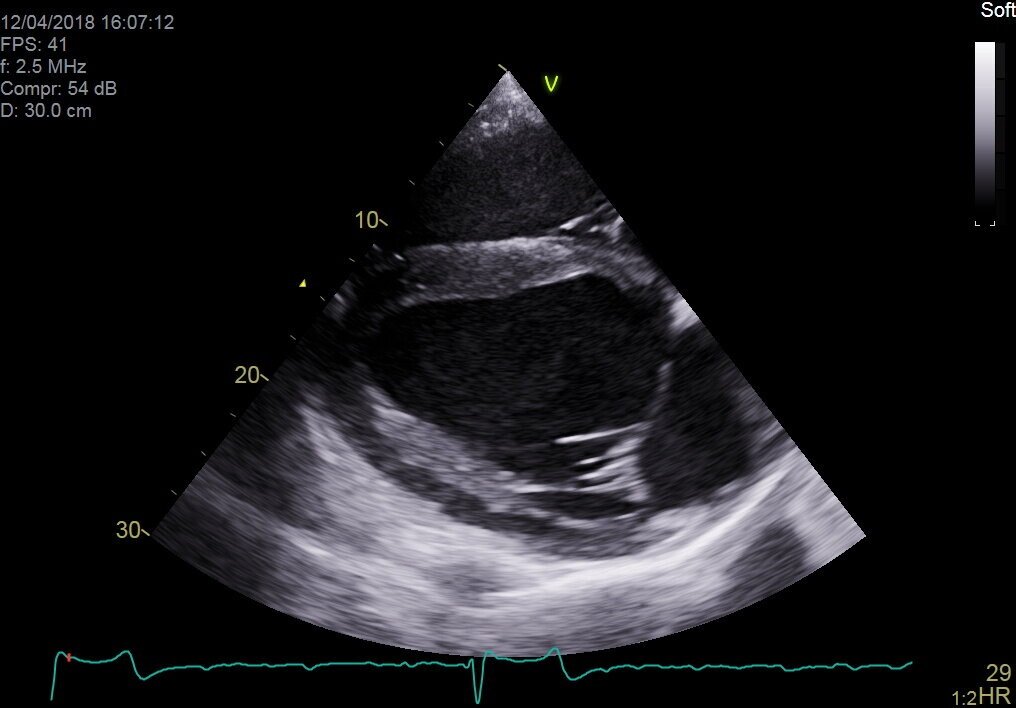
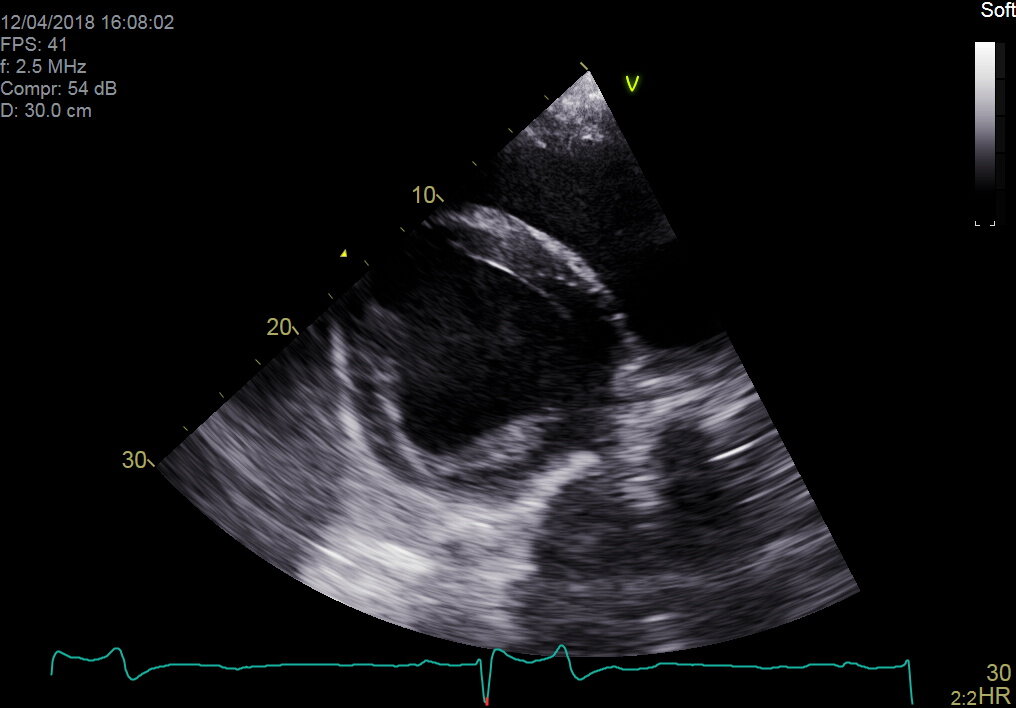
Veterinarians use a combination of the information you tell them, their observation of the horse and the barn, and a careful physical and respiratory examination that often involves “rebreathing.” This is a technique where a bag is briefly placed over the horse’s nose, causing them to breathe more frequently and more deeply to make their lungs sound louder. This helps your veterinarian hear subtle changes in air movement through the lungs and amplifies the wheezes and crackles that characterise a horse experiencing a severe asthma attack. Wheezes indicate air “whistling” through constricted airways, and crackles mean airway fluid buildup. The fluid accumulation is caused by airway inflammation and contributes to the challenge of getting air into the lung.
Other tests your veterinarian might use are endoscopy, bronchoalveolar lavage, and in the specialist setting, pulmonary function testing. They will also perform a complete blood count and biochemical profile assay to help rule out the presence of an infectious disease.
Endoscopy allows your veterinarian to see the mucus in the trachea and large airways of the lung. It also lets them see whether there are physical changes to the shape of the airways, which can be seen in horses with sEA.
Bronchoalveolar lavage, or “lung wash” is how your veterinarian assesses whether there is an accumulation of mucus and inflammatory cells in the smallest airways that are too deep in the lung to be seen using the endoscope. Examining lung wash fluid is a very important way to differentiate between the different types of mEA, between sEA in remission and an active asthma attack, and conditions like pneumonia or a viral lung infection.
Finally, if your veterinarian is from a specialty practice or a veterinary teaching hospital, they might also perform pulmonary function testing. This allows your veterinarian to determine if your horse’s lungs have hyperreactive airways (the hallmark of asthma), lung stiffening, and a reduced ability to breathe properly.
Results from these tests are crucial to understanding the severity and prognosis of the condition. As noted earlier, mEA can go away on its own; but medical intervention may speed healing and the return to athletic performance. With sEA, remission from an asthmatic flare is the best we can achieve. As the disease gets worse over time, eventually the affected horse may need to be euthanised.
Management, Treatment and Most Importantly—Prevention
Successful treatment of mEA and sEA flares, as well as long-term management, requires a multi-pronged approach and strict adherence to your veterinarian’s recommendations.

Rest is important because forcing your horse to exercise when they are in an asthma attack further damages the lung and impedes healing. To help avoid lung damage when smog or forest-fire smoke is high, a very useful tool is your local, online, air quality index (just search on the name of your closest city or town and “AQI”). Available worldwide, the AQI gives advice on how much activity is appropriate for people with lung and heart conditions, which are easily applied to your horse. For example, if your horse has sEA and if the AQI guidelines say that asthmatic people should limit their activity, then do the same for your horse. If the AQI says that the air quality is bad enough that even healthy people should avoid physical activity, then do the same for you AND your horse. During times of poor air quality, it is recommended to monitor the AQI forecast and plan to bring horses into the barn when the AQI is high and to turn them out once the AQI has improved.
Prevent dusty air. Think of running your finger along your tack box – whatever comes away on your finger is what your horse is breathing in. Reducing dust is critical to preventing the development of mEA and sEA, and for managing the horse in an asthmatic flare.
Logical daily practices to help reduce dust exposure:
Turn out all horses before stall cleaning
Wet down the aisle prior to sweeping
Never sweep debris into your horse’s stall
Use low-dust bedding like wood shavings or dust-extracted straw products, which should also be dampened down with water
Reduce arena, paddock, and track dust with watering and maintenance
Consider low-dust materials when selecting a footing substrate
Steam (per the machine’s instructions) or soaking hay (15–30 minutes and then draining, but never store steamed or soaked hay!)
Feed hay from the ground
Feed other low-dust feeds
Avoid hay feeding systems that allow the horse to put their nose into the middle of dry hay—this creates a “nosebag” of dust

Other critical factors include ensuring that the temperature, humidity and ventilation of your barn are seasonally optimised. Horses prefer a temperature between 10–24 ºC (50–75 ºF), ideal barn humidity is between 60–70%. Optimal air exchange in summer is 142 L/s (300 cubic feet/minute). For those regions that experience winter, air exchange of 12–19 L/s (25–40 cubic feet/minute) is ideal. In winter, needing to strip down to a single layer to do chores implies that your barn is not adequately ventilated for your horse’s optimal health. Comfortable for people is often too hot and too musty for your horse!
Medical interventions for controlling asthma are numerous. If your veterinarian chooses to perform a lung wash, they will tailor the drug therapy of your asthmatic horse to the results of the wash fluid examination. Most veterinarians will prescribe bronchodilators to alleviate airway constriction. They will also recommend aerosolised, nebulised or systemic drugs (usually a corticosteroid, an immunomodulatory drug like interferon-α, or a mast cell stabilisers like cromolyn sodium) to manage the underlying inflammation. They may also suggest nebulising with sterile saline to help loosen airway mucus and may suggest feed additives like omega 3 fatty acids, which may have beneficial effects on airway inflammation.
New Research and Future Directions
Ongoing research is paramount to expanding our knowledge of what causes equine asthma and exploring innovative medical solutions. Scientists are actively investigating the effects of smog and barn dusts on the lungs of horses. They are also working to identify new targeted therapies, immunotherapies and other treatment modalities to improve outcomes for affected horses.
Conclusion

Both mild and severe equine asthma are caused and triggered by the same air pollutants, highlighting the need for careful barn management. The alarming rise in air pollution levels poses an additional threat to equine respiratory health. Recognising everyday coughs as potential warning signs and implementing proper diagnostic tests, day-to-day management practices and medical therapies are crucial in combating equine asthma. By prioritising the protection of our horse’s respiratory health and staying informed about the latest research, we can ensure the well-being of our equine companions for years to come.
Bleeders - the facts, fiction and future direction
By Dr. David Marlin

We are now approaching half a century since Bob Cook pioneered the use of the flexible fibreoptic endoscope, which allowed examination of the respiratory tract in the conscious horse. One of the important outcomes of this technique was that it opened the door to the study of ‘bleeding’ or exercise-induced pulmonary haemorrhage (EIPH). But nearly 50 years on the irony is perhaps that whilst we have become good at describing the prevalence of EIPH and some of the factors that appear to increase the severity of EIPH within individual horses, we still lack a clear understanding of the condition and how to manage it. I use the term manage rather than treat or prevent as our knowledge of EIPH must show us that EIPH cannot be stopped entirely; it is a consequence of intense exercise. The other irony is that in the past 50 years, by far the majority of research into the management of EIPH has focussed on the use of the diuretic furosemide. Whilst we have good evidence from controlled studies that furosemide reduces the severity of EIPH on a single occasion, we still lack good evidence to suggest that furosemide is effective when used repeatedly during training and or racing; and there is also evidence to the contrary.
Let’s review some basic facts about EIPH, which should not be contentious.
EIPH is the appearance of blood in the airways associated with exercise.
EIPH occurs as a result of moderate to intense exercise. In fact, EIPH has been found after trotting when deep lung wash (bronchoalveolar lavage or BAL) is done after exercise.
EIPH most often involves the smallest blood vessels (capillaries) but can sometimes and less commonly be due to the rupture of larger blood vessels.
The smallest blood vessels are extremely thin. Around 1/100th the thickness of a human hair. But this extremely thin membrane is also what allows racehorses such as thoroughbreds, standardbreds and Arabs to use oxygen at such a high rate and is a major reason for their athleticism.
EIPH is a progressive condition. The chance of seeing blood in the trachea after exercise increases with time in racing.
EIPH is variable over time, even when horses are scoped after the same type of work.
If you ‘scope a horse after three gallops in a row, you can expect to see blood in the trachea on at least one occasion.
EIPH damage to the lungs starts at the back and top, and over time moves forward and down and is approximately symmetrical.
Following EIPH the lung becomes fibrotic (as scar tissue), stiffer and does not work as well. The iron from the blood is combined with protein and stored permanently in the lung tissue where it can cause inflammation.
High blood pressure within the lung is a contributing factor in EIPH. Horses with higher blood pressure appear to suffer worse EIPH.
There is also evidence that upper airway resistance and breathing pattern can play a role in EIPH.
Airway inflammation and poor air quality may increase the severity of EIPH within individual horses.
Increasing severity of EIPH appears to have an increasing negative effect on performance.
Visible bleeding (epistaxis) has a very clear and marked negative effect on performance.
In order to make progress in the management of EIPH (i.e., to minimise the severity of EIPH in each individual), there are certain steps that trainers can take based on the information we have to date.
These include:

Ensuring good air quality in stables
Regular respiratory examination and treatment of airway inflammation
Reduced intensity of training during periods of treatment for moderate to severe airway inflammation
Extended periods of rest and light work with a slower return to work for horses following viral infection
Addressing anything that increases upper airway resistance (e.g., roaring, gurgling)
Avoiding intense work in cold weather
Avoiding extremes of going
Limiting number of training days in race preparation and increasing interval between races

Endoscopy
FUTURE OPPORTUNITIES IN UNDERSTANDING AND MANAGING EIPH
We have to accept EIPH as a normal consequence of intense exercise in horses. Our aim should be to reduce the severity to a minimum in each individual horse. However, there are areas in which we still need a much greater scientific understanding.
What actually causes the capillaries to leak or rupture?…
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Thoroughbred Sales Assessment; Update from the Gerald Leigh Memorial Lectures, 2019
By Tom O’Keeffe

The Beaufort Cottage Educational Trust Gerald Leigh Memorial Lectures took place this year at the National Horseracing Museum in Newmarket and a host of international and local veterinary specialists and industry leaders were present to discuss the veterinary aspects of the sales selection of the thoroughbred.
Gerald Leigh was a prominent breeder and racehorse owner until his death in 2002; and his friend and vet Nick Wingfield Digby opened the seminar and introduced the speakers. The Gerald Leigh Charitable Trust has established this annual lecture series to provide a platform for veterinary topics relating to the thoroughbred to be discussed amongst vets and prominent members of the industry.
Sir Mark Prescott described his take on the sales process and some of the changes he has noted since his early involvement in the industry. He recalled how the first Horses in Training sale he attended had only 186 horses. In those early days, his role was to sneak around the sales ground stables late at night on the lookout for crib biters. Back then, there was no option to return horses after sale, and as a result, trainers preferred to buy horses from studs they were familiar with—a policy Sir Mark still follows to this day.
Sir Mark went on to explain that he believes strongly that the manner in which an animal is reared has a strong bearing on their ability to perform at a later date. Sir Mark also mentioned that horses can cope with many conformational faults nowadays that would have been deemed unacceptable in his early years. He attributed this to improvements in ground conditions, such as watering and all-weather surfaces. Mike Shepherd, MRCVS, of Rossdales Equine Practice in Newmarket had been tasked with describing and discussing the sales examination from a veterinary viewpoint and in particular attempting to define what vets are trying to achieve in this process.
Shepherd’s key message was that the physical exam is the cornerstone of any veterinary evaluation. A vet examining a horse on the sales ground is not a guarantee that the horse will never have an issue—there is no crystal ball. Owners and trainers should be aware there are several limitations of the vetting process, and it is helpful to think in terms of a “pre-bid inspection” rather than a “pre-purchase examination”. The horse is away from its home environment, and this puts a lot of stress on the animal. In most cases, pre-purchase exercise is not possible, so conditions that are only apparent when the horse is exercising and in training may go undetected.
Time is a major challenge, with both vendors and prospective purchasers pushing for everything to be done as quickly as possible. A busy sales vet may have a long list of horses to examine, and information on each must be transferred to their client coherently and clearly—all before the horse is presented for sale. It can be challenging to acquire a detailed veterinary history. Previous surgeries, medication and vices displayed by the animal ought to be reported, but in many cases the person with the horse is not in a position to accurately answer questions on longer-term history.
Everyone involved—the vendor, the prospective purchaser, and the auction house—wants the process to go ahead. The horse to be bought/sold and the vet can be seen as a stumbling block. Prospective purchasers may want the horse to be examined clinically, its laryngeal function examined by endoscope, radiographs of the horse’s limbs either reviewed or taken, ultrasound examinations of their soft tissue structures and heart performed. The role of the vet is to help the purchaser evaluate all this information and make an evidence-based decision on whether to purchase the horse.
Examining vets can face conflicts of interest when examining horses that are under the ownership or care of one of their clients. Shepherd explained how Rossdales, and some other practices involved in sales work, have a protocol that an examining vet will not perform a vetting on a horse in the care of one of their own clients, and will disclose to the prospective purchaser if the vendor is a client of the practice. It is crucial to avoid working for both buyer and seller as a conflict of interest becomes unavoidable.
It is also essential that the vet understands exactly what the horse is expected to do following the sale. Thoroughbred horses in flat racing have short timescale targets and, as a result, certain parts of the examination carry more weight than others. For example, the knees and fetlock joints are commonly implicated in lameness in flat racehorses; thus particular attention must be paid to these joints when examining yearlings. Soft tissue injuries are impactful in all young thoroughbreds, but there is a particular emphasis on tendon integrity in the National Hunt racehorse because career-threatening tendon injuries are particularly prevalent in these horses. When evaluating potential broodmares, good feet are very relevant, and overall conformation is particularly important if the aim is to breed to sell. Vetting horses for clients aiming to pin hook their purchases places different requirements on the examining vet. These horses need to be able to cope with the preparation required for another sale, and they must also stand up to the scrutiny of vets at a later sale. The horse’s walk and conformation rank high in the foal/ yearling stage but may be judged to be less significant if the horse breezes in a fast time at a breeze up sale.
It is also critical that purchasers recognise that many of the common veterinary issues encountered in training are not detectable at the Sales stage. …