Assessment of historical worldwide fracture & fatality rates and their implications for thoroughbred racing’s social licence

Article by Ian Wright MRCVS
Racing’s social licence is a major source of debate and is under increasing threat. The principal public concern is that racing exposes horses to significant risk of injury including catastrophic (life-ending) injuries of which fractures are the commonest cause. The most recent studies in the UK indicate that fractures account for approximately 75% of racecourse fatalities. Recent events highlight the need for urgent stakeholder discussion, which necessarily will be uncomfortable, in order to create cogent justification for the sport and reliant breeding industry.

A necessary prelude to discussion and debate is an objective assessment of risk. All and any steps to reduce risks and mitigate their impact are important and must be embraced by the horseracing industry (and quite possibly all other horse sports). To begin this, a here and now assessment is important: put simply, does the price paid (risk) justify the benefit (human pleasure, culture, financial gain, employment, tax revenue, etc). Objective data provides perspective for all interested parties and the voting public via their elected representatives, who ultimately provide social licence, with other welfare issues—both human and animal—on which society must pass judgement.
The data in Tables 1 to 12 report a country by country survey of fracture and fatality rates reported in scientific journals and documented as injuries/fatalities per starters. It may be argued that little of the data is contemporary; the studies range from the years 1980 to 2013. However, the tabulated data provided below is the most up to date that can be sourced from independently published, scrutinised scientific papers with clear—albeit sometimes differing—metric definitions and assessable risk rates.

In assimilating and understanding the information, and in order to make comparisons, some explanatory points are important. The first, and probably the most important, is identification of the metric. Although at first glance, descriptor differences may appear nuanced, what is being recorded massively influences the data.
These include fatality, catastrophic injury, fracture, orthopaedic injury, catastrophic distal limb fracture, fatal musculoskeletal injury, serious musculoskeletal injury, and catastrophic fracture. The influence of the metric in Japanese racing represents the most extreme example of this: ‘fracture’ in the reporting papers included everything from major injuries to fragments (chips) identified after racing in fetlocks and knees, i.e. injuries from which recovery to racing soundness is now an expectation. At the opposite pole, studies in other countries document ‘catastrophic’, i.e. life-ending fractures which have a substantially lower incidence. The spectrum of metric definitions will all produce different injury numbers and must be taken into account when analysing and using the data.
Studies also differ in the methods of data collection that will skew numbers in an undetermined manner. Some only record information available at the racecourse, others by identifying horses that fail to race again within varying time periods, horses requiring hospitalisation following racing, etc. The diagnostic criteria for inclusion of horses also vary between reports: some document officially reported incidents only, some are based only on clinical observations of racecourse veterinary surgeons, while others require radiographic corroboration of injuries.
From a UK perspective, the data is quite robust in concluding that risks differ significantly between race types. The majority of fractures that occur in flat racing, and between obstacles in jump racing, are the result of stress or fatigue failure of bone. They are not associated with traumatic events, occur during high speed exercise, are site specific and have repeatable configurations. In large part these result from a horse’s unique athleticism: in the domesticated species, the thoroughbred racehorse represents the pinnacle of flight-based evolution. Fractures that result from falls in jump racing are monotonic—unpredictable, single-event injuries in which large forces are applied to bone(s) in an abnormal direction.

This categorisation is complicated slightly as fatigue failure at one site, which may be bone or supportive soft tissue, can result in abnormal loads and therefore monotonic fracture at another. The increased fracture rate in jump racing is explained in part by cumulative risk. However, it is complicated by euthanasia of horses with injuries with greater post injury commercial value and/or breeding potential that might be treated. Catastrophic injuries and fatality rates in NH flat races are most logically explained by a combination of the economic skew seen in jump racing and compromise of musculoskeletal adaptation.
Racing surface influences both injury frequency and type. Studies in the UK have consistently documented an increased fatality rate and incidence of lower limb injury on synthetic (all weather) surfaces compared to turf. Although risk differences are clear, confounding issues, such as horse quality and trainer demographic, mean that the surface per se may not be the explanation. In the United States, studies reporting data from the same geographic location have produced mixed results. In New York, these documented greater risks on dirt than turf surfaces; while a California study found no difference, and a study in Florida found a higher risk on turf. A more recent study gathering data from the whole of the U.S. reported an increased risk on dirt surfaces. Variations in the nature of injury between surfaces may go some way toward explaining fatality differences.
Much has been done to reduce recognisable risk factors particularly in jump racing; but in the UK, it is likely (for obvious data supported reasons) that it will come under the greatest scrutiny. The incidence of fractures and fatalities in flat racing are low, and the number of currently identified risk factors are high. Over 300 potential influences have been investigated, and over 50 individual factors demonstrated statistically are associated with increased risk of catastrophic injury.
The majority of fractures occurring in flat racing (and non-fall related fractures in jump racing) are now also treatable, enabling horses to return to racing and/or to have other comfortable post-racing lives.

The common public presumption that fractures in horses are inevitably life-ending injuries is a misconception that could readily be remedied. An indeterminate number of horses are euthanised on the basis of economic viability and/or ability to care for horses retired from racing. On this point, persistence with a paternalistic approach is a dangerous tactic in an educated society. Statements that euthanasia is ‘the kindest’ or ‘best’ thing to do, that it is an ‘unavoidable’ consequence of fracture or that only ‘horsemen understand or know what is best’ can be seen as patronising and will not stand public scrutiny.
At some point, data to distinguish between horses euthanised as a result of genuinely irreparable injuries and those with fractures amenable to repair will become available. Before this point is reached, the consequences require discussion and debate within the racing industry.
Decisions on acceptable policies will have to be made and responsibility taken. In its simplest form, this is a binary decision. Either economic euthanasia of horses, as with agricultural animals, is considered and justified as an acceptable principle by the industry or a mechanism for financing treatment and lifetime care of injured horses who are unlikely to return to economic productivity will have to be identified. The general public understands career-ending injuries in human athletes: These appear, albeit with ongoing development of sophisticated treatments at reducing frequency, in mainstream news.
Death as a direct result of any sporting activity is a difficult concept in any situation and draws headlines. Removal of the treatable but economically non-viable group of injuries from data sets would reduce, albeit by a currently indeterminate number, the frequency of race course fatalities. However, saving horses' lives whenever possible will not solve the problem: it will simply open an ethical debate viz is it acceptable to save horses that will be lame? In order to preserve life, permanent lameness is considered acceptable in people and is not generally considered inhumane in pets. Two questions arise immediately: (i) How lame can a horse be in retirement for this to be considered humane? (ii) Who decides? There is unquestionably a spectrum of opinion, all of which is subjective and most of it personal. It will not be an easy debate and is likely to be complicated further by consideration of sentience, which now is enshrined in UK law (Animal Welfare (Sentience) Act 2022); but it requires honest ownership of principles and an agreed policy.
For the avoidance of doubt, while the focus of this article and welfare groups’ concerns are on racecourse injuries, those sustained in training follow a parallel pathway. These currently escape attention simply by being, for the most part, out of sight and/or publicity seeking glare.
Within racing, there is unquestionably a collective desire to minimise injury rates. Progress has been made predominantly by identification of extrinsic (i.e. not related to the individual horse) risk factors followed by logical amendments. In jump racing (monotonic fractures), obstacle modification, re-siting and changing ground topography are obvious examples of risk-reducing measures that have been employed.
In flat racing progress has involved identification risk factors such as race type and scheduling, surface, numbers of runners, track conditions etc which have guided changes. However, despite substantial research and investment, progress in identification of intrinsic (ie relating to the individual horse) risk factors is slow. While scientifically frustrating, a major reason for this is the low incidence of severe fractures: this dictates that the number of horses (race starters) that need to be studied in order to assess the impact of any intervention is (possibly impractically) high. Nonetheless, scientific justification is necessary to exclude a horse from racing and to withstand subsequent scrutiny.
Review of potential screening techniques to identify horses at increased risk of sustaining a fracture while racing is not within the scope of this article, but to date none are yet able, either individually or in combination, to provide a practical solution and/or sufficiently reliable information to make a short-term impact. It is also important to accept that the risk of horses sustaining fractures in racing can never be eliminated. Mitigation of impact is therefore critical.
When fractures occur, it is imperative that horses are evaluated to be given the best possible on course care. This may, albeit uncommonly be euthanasia. Much more commonly, horses can be triaged on the course and appropriate support applied before they are moved to the racecourse clinical facility for considered evaluation and discussion. The provision of fracture support equipment to all British racecourses in 2022 marked a substantial step forward in optimising injured horse care.
Neither racing enthusiasts nor fervent objectors are likely to change their opinions. The preservation of social licence will be determined by the open-minded majority who lie between: it is the proverbial ‘man on the street’ who must be convinced. The task of all who appreciate horse racing's contributions to society and wish to see it continue is to remain focussed on horse welfare, if necessary to adjust historical dogmas, absorb necessary costs and to encourage open, considered, honest (factually correct) risks versus benefits discussion.

Equine Neck CT: Advancing diagnostic precision in racehorses
Article by Rachel Tucker MRCVS

Introduction
When considering neck disorders in the racehorse, we most commonly think of severe conditions such as acute neck trauma and cervical vertebral myelopathy (Wobbler Syndrome). These represent the most severe end of the scale of orthopaedic and neurologic injury to the neck; and a diagnosis, or at least prognosis, is usually clear. However, neck conditions encompass a far wider range of clinical presentations.

Horse positioned in ct scanner
At the milder end of the scale, signs may be subtle and easily missed, whilst still being responsible for discomfort and reduced performance. The recent ability to perform a computed tomography (CT) scan of a horse’s neck represents a major advancement in our ability to diagnose neck conditions. Timely and accurate diagnosis allows efficient and targeted treatment, the ability to plan schedules and improvement in welfare through the provision of appropriate treatment and earlier return to function.
In neurologic cases, an accurate diagnosis facilitates risk management for both the horse, their handlers and riders, while improving safety for all. As conditions and injuries of the neck are being better characterised using CT, new medical and surgical treatment options are being developed, giving the potential for improved outcomes and fewer losses from the racing industry.
This article summarises how CT is being increasingly used by vets to diagnose conditions of the neck and how it is revealing previously unknown information and providing exciting new treatment opportunities.
Presentation
Conditions of the neck can cause a range of signs in the horse, which are wide-ranging in their presentation and variable in their severity. The manner in which these conditions present depends on which anatomical structures are affected. Issues affecting the bones, joints and/or soft tissues of the neck can all cause neck pain, which can manifest in a number of ways. Cases of neck pain can be severe, resulting in a horse with a rigid, fixed neck carriage, an unwillingness to walk and struggling to eat, perhaps due to a traumatic event. Neck fractures are thankfully uncommon but can be catastrophic.

More moderate signs might be displayed as a stiff neck, with reduced range of movement and resentment of ridden work. There may be pain on palpation of the neck and changes in the neck musculature. Increasingly, we are seeing horses with far more subtle signs, which are ultimately revealed to be due to neck pain and neck pathology. Typically, these horses might have an acceptable range of motion of their neck under most circumstances, but they suffer pain or restriction in certain scenarios, resulting in poor performance. This may be seen as tension through the neck, resisting rein contact, a reluctance to extend the neck over fences, or they may struggle on landing.
Riders might report a feeling of restriction or asymmetry in the mobility of the neck. In addition, these horses may be prone to forelimb tripping or show subtle forelimb lameness.
Any condition, which causes injury or disease to the spinal cord or nerves within the neck, also causes a specific range of neurologic signs. Compression of the spinal cord is most commonly caused by malformations or fractures of the cervical vertebrae, or enlargement of the adjacent articular process (facet) joints. This results in classic ‘Wobbler’ symptoms, which can range from subtle weakness and gait abnormalities, through to horses that are profoundly weak, ataxic and uncoordinated. This makes them prone to tripping, falling, or they may even become recumbent.
Peripheral nerve deficits are uncommon but become most relevant if they affect the nerves supplying the forelimbs, which can result in tripping, forelimb lameness, or local sensory deficits. This lameness might be evident only in certain circumstances, such as when ridden in a rein contact. This lameness is difficult to pinpoint as there will be no abnormality to find in the lame limb, indeed a negative response to nerve and joint blocks (diagnostic analgesia) will usually be part of the diagnostic process.
Horses can present with varying combinations and severities of neck pain, neurologic signs and peripheral nerve deficits, creating a wide range of manifestations of neck related disease.
Diagnosis
A diagnosis of neck pain is based on careful static and dynamic clinical examination and may be supported by seeing a positive response to treatment. Neurologic deficits are noted during a specific neurologic assessment, which includes a series of provocation tests such as asking a horse to walk over obstacles, back up, turn circles and walk up and down a hill. Confirming neck pathology as the cause of signs can be difficult. Until recently, radiography has been the mainstay imaging modality. Radiographs are useful for assessment of the cervical vertebrae and continue to play an important role in diagnosis; however the complex 3-dimensional shape of these bones, the large size of the neck and an inability to take orthogonal (right-angled) x-ray views means that this 2-dimensional imaging modality has significant limitations. High quality, well-positioned images are essential to maximise the diagnostic potential of radiographs.
A turning point in our diagnostic ability and understanding of neck dysfunction has been the recent adaptation of human CT scanners to allow imaging of the horse’s neck. A number of equine hospitals across the United Kingdom and Northern Europe now offer this imaging modality. We have been providing this service at Liphook Equine Hospital since 2017, with over 150 neck scans performed to date.
The CT procedure
A computed tomography (CT) scan combines a series of x-ray images taken from different angles around the area of interest to create a 3-dimensional volume of imaging data. This data is presented as a grayscale image which can be viewed in any plane and orientation. It provides excellent bone detail, and post processing techniques can provide information on soft tissue structures too. Additional techniques can be employed such as positive contrast myelography to provide greater detail about soft tissue structures. Myelography delineates the spinal cord using contrast medium injected into the subarachnoid space and is indicated in any case showing neurologic signs suggestive of spinal cord compression.
Neck CT is performed under a short general anaesthetic. Scans without myelography typically take less than 20 minutes to complete. The entire neck is imaged, from the poll to the first thoracic vertebra. The procedure is non-invasive and low risk, with anaesthetic-related complication presenting the main risk factor to the procedure. We have not encountered any significant complications in our plain CT scan caseload to date. Horses showing ataxia, weakness and incoordination (Wobbler’s), undergo CT myelography which adds around 20 minutes to the procedure. These horses are exposed to a greater level of risk due to their neurologic condition, the injection of a contrast agent and the increased chance of destabilising a more severe lesion during the procedure.
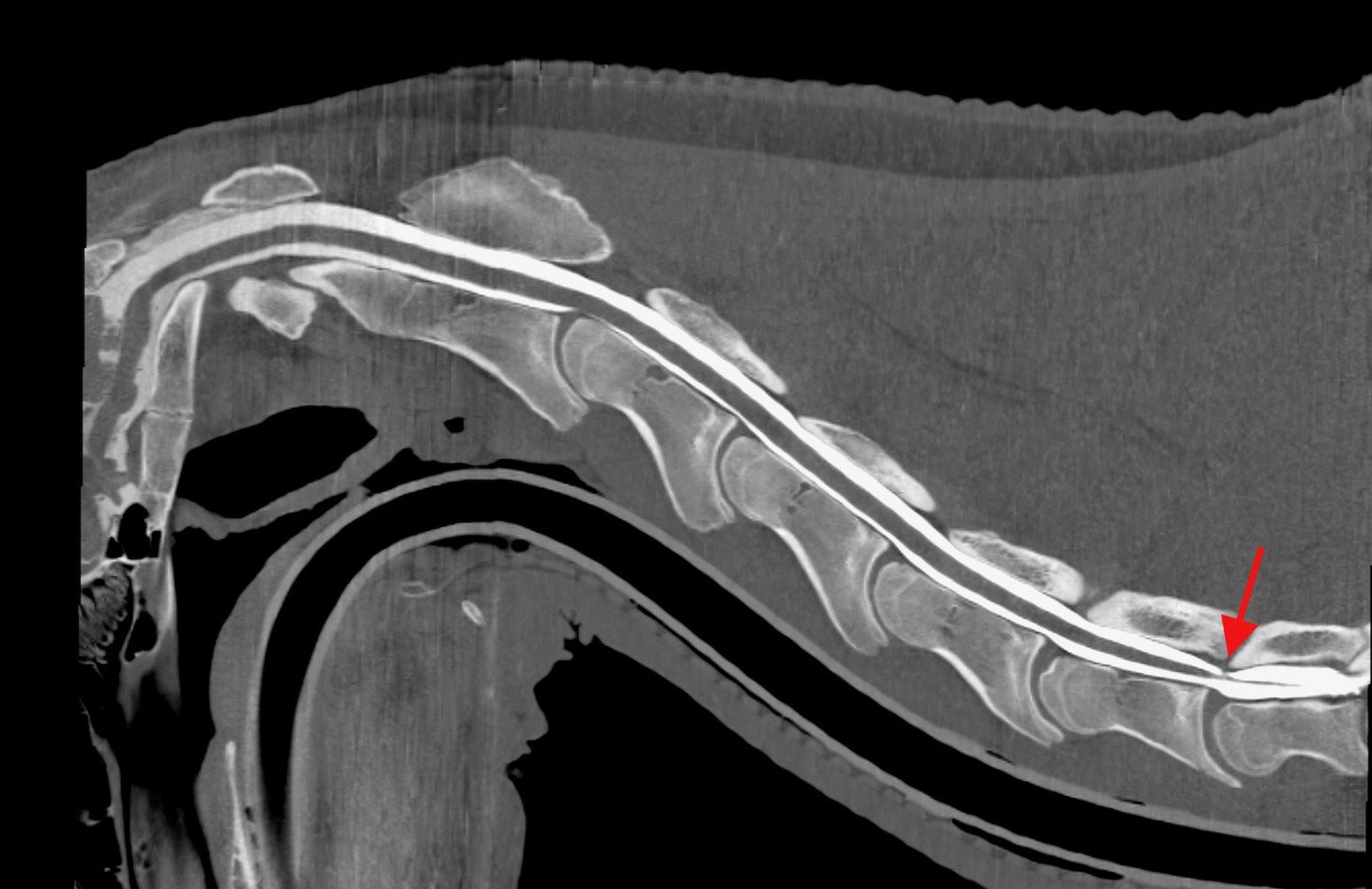
Sagittal and transverse CT myelogram images of a young racing thoroughbred showing neurologic (Wobbler) signs. shows narrowing of the spinal canal at the base of the neck (arrow)
CT is revealing more detailed information about ways that spinal cord compression can occur in Wobbler cases, about compression of spinal nerves resulting in forelimb gait deficits and precise detail about fracture configurations. It gives us detailed images of articular process joint disease, intervertebral disc disease, developmental conditions and anatomic variations. It is also revealing information about rare diseases such as vertebral abscesses or spinal neoplasia. As our caseload and confidence in the imaging modality grows, we are learning more about the value of CT in examining more subtle neck conditions. We are also bringing the benefit of a more accurate diagnosis, allowing precise targeted treatment and a better ability to provide a prognosis about outcomes—likely progression or safety factors. CT myelography allows circumferential imaging of the spinal canal and yields significantly more information than traditional x-ray myelography. As a result, we hope to enable better case selection of horses that may benefit from Wobbler surgery, with the goal of resulting in improved success rates of the surgery.
Innovations in treatment

image shows a fracture of the articular process of the 3rd cervical vertebrae in the mid neck, which was not visible on x-ray.
New treatment options are emerging as a result of our more accurate diagnoses of neck pathology. Of the first 55 horses which underwent neck CT at our hospital, we were surprised to discover that 13 (24%) had some form of osteochondral fragmentation within the articular process joints of their neck. Some of these horses were young Thoroughbreds, bred to race but showing Wobbler signs. These tended to have convincing CT evidence of type 1 CVM (Wobbler Syndrome) and osteochondrosis affecting their neck. Others had fragments which were larger and more discrete, with evidence of articular process joint enlargement/arthritis but no other bony lesions. These horses were typically older and of a range of breeds and uses.
In those horses presenting with signs of neck pain but no neurologic deficits, surgical removal of these fragments was proposed. Following further consideration and cadaver training, we have begun to offer this surgery for horses that fit the appropriate criteria and have surgically accessible fragments. We have performed arthroscopic or arthroscopic-assisted fragment removal from eight articular process joints in six horses to date. No intraoperative or postoperative complications have been encountered; and five of six horses showed complete resolution of neck pain. In the sixth horse, full recovery was not anticipated due to the presence of additional neck pathology, but partial improvement occurred for two years. Fragment removal has relieved signs of neck pain and stiffness and caused improved performance in these horses.
Two procedures that are emerging to treat spinal nerve root impingement are a targeted peripheral nerve root injection and a keyhole surgical procedure to widen the intervertebral foramen. Nerve root injection is performed in the standing sedated horse under ultrasound guidance. Surgery is performed under anaesthesia, using specialised minimally invasive equipment to widen the bony foramen using a burr. This surgery is in its infancy but offers an exciting treatment option.
Additionally, CT gives us the ability to better plan for fracture repair, undoubtedly improving our case selection for Wobbler surgery; it more accurately guides intra-articular injection of the articular process joints.
Summary
Computed tomography is transforming our ability to diagnose conditions of the horse’s neck. The procedure is low risk and now widely available in the UK and other parts of Europe. It is driving the innovation of novel treatment options with the goal of improving outcomes and reducing losses to conditions of the neck. Our CT findings are posing new questions about neck function, pain and neurologic disease and is an active area of ongoing research.
Anatomy of the cervical vertebrae

The neck vertebrae of the horse
The neck consists of seven cervical vertebrae which form a gentle S-shaped curve to link the skull at the poll to the thoracic vertebrae of the chest. Its primary functions are to protect the spinal cord, support the heavy weight of the head and to allow a large range of movement so that a horse can monitor his environment and run at speed, both being vital to this prey species.
The first (atlas) and second (axis) cervical vertebrae are highly adapted to allow head mobility. The third to sixth vertebrae are very similar in shape, whereas the seventh is shortened as it starts to show similar features to the vertebrae of the thorax. The typical cervical vertebra consists of a cylindrical column of bone (vertebral body) articulating with adjacent vertebrae via an intervertebral disc.
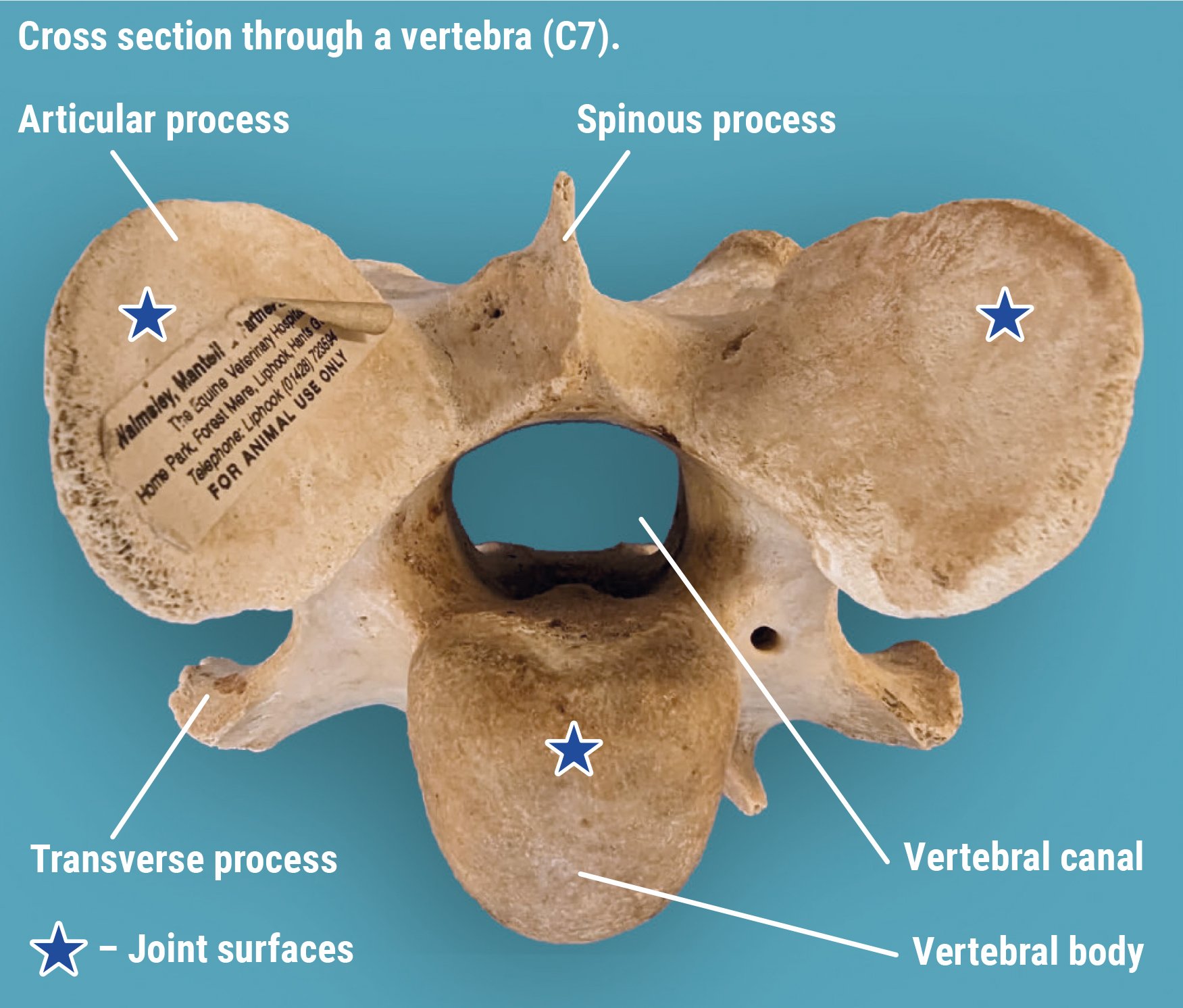
Running along the upper surface of this bony column is a bony canal created by the vertebral arch. This canal protects the spinal cord and associated structures that run through the centre. Above and to the side of the spinal canal sit the paired articular processes and below; and to the side sit the transverse processes. These are bony prominences to which muscles attach. The soft tissues of the neck are complex and intrinsically linked to the forelimbs and entire axial skeleton.
The articular processes also form the articular process joints (facet joints) which create an additional two joints between each vertebra. Although highly adapted, these joints are similar to others in the body consisting of cartilage-lined surfaces, a joint capsule and joint fluid. The joint surfaces are oval in shape, approximately 3-4cm in diameter and sit at an oblique angle to the neck. They provide important additional support and mobility to the neck.
References:
Schulze N., Ehrle, A., Beckmann, I and Lischer, C. (2021) Arthroscopic removal of osteochondral fragments of the cervical articular process joints in three horses. Vet Surg. ;1-9.
Swagemakers J-H, Van Daele P, Mageed M. Percutaneous full endoscopic foraminotomy for treatment of cervical spinal nerve compression in horses using a uniportal approach: Feasibility study. Equine Vet J. 2023.
Tucker R, Parker RA, Meredith LE, Hughes TK, Foote AK. Surgical removal of intra-articular loose bodies from the cervical articular process joints in 5 horses. Veterinary Surgery. 2021;1-9.
Wood AD, Sinovich M, Prutton JSW, Parker RA. Ultrasonographic guidance for perineural injections of the cervical spinal nerves in horses. Veterinary Surgery. 2021; 50:816–822.