Funding research in equine veterinary development - the financial impact of the pandemic on scientific research

By Annie Dodd
Something we can all agree on is that 2020 has not gone as planned. Nothing has escaped the effects of COVID-19, and as far as the racing industry is concerned, that goes for scientific research as well as the day-to-day activity in training centres, on studs and on the track.
Amongst the statutory duties of the Horserace Betting Levy Board (HBLB) is a requirement to apply funds for the advancement of veterinary science and education. In a normal year, the Board, through its Veterinary Advisory Committee, would be inviting applications for new projects to start the following year, as well as managing work already underway.
In 2020, access to university labs and field work has been severely restricted, meaning that many of the ongoing projects are being delayed—a frustrating situation for all. Everything will be finished, but it will take longer than planned.
The financial impact of the pandemic on racing is well known. For the Levy Board, many of the non-racing budget items have had to be restricted, and this has included veterinary science and education. For the first time there has been no grant call this year, and so no new work will be starting in 2021.
The better news is that three new major projects, 12 small projects, one research scholarship and two post-doctoral fellowships have begun in 2020.
The major research projects are hosted by institutions such as university veterinary schools. These can go up for up to three years, with budgets normally in the region of £200,000 to £300,000. …
CLICK HERE to return to issue contents.


BUY THIS ISSUE IN PRINT OR DOWNLOAD
Bowed tendons - different treatment options - new ultrasound technology - ultrasound tissue characterisation

By Sarah Plevin
Overstrain injuries to the superficial digital flexor tendon (SDFT) are among the most common musculoskeletal injuries for all athletic equine disciplines but account for a significant amount of wastage in the Thoroughbred (TB) racehorse.
Treatment options for such ‘bowed tendons’ are many and varied, but all have a couple of things in common: time out of training; expense and no guarantee of success.
It makes sense then, that prevention of injury should always be the goal, and failing that, a method to optimally guide rehabilitation is needed.
Unfortunately, limitations of current imaging diagnostics have restricted their use for accurately monitoring the tendon.
A new ultrasound technology, however, called ultrasound tissue characterisation, may get us one step closer to achieving the goals of injury prevention and optimal rehabilitation.
What would the ideal tendon imaging modality allow us to do?
Monitor the effects of exercise on the tendon
Early detection of overstrain injuries
Be able to stage the lesion, i.e., determine the level of degenerative change within the tendon structure
Fine-tune therapy
Guide rehabilitation
Why are tendon injuries so tricky?

Figure 1: Functionally normal healthy aligned tendon bundles.
A normal healthy tendon is made from aligned organized tendon bundles. (Figure 1) Deterioration of this structure ranges on a spectrum from complete disruption (core lesion) to more minor changes, but all affect the ability of the tendon to function optimally.
Degenerative changes within the tendon matrix are not uniform—meaning that not all overstrain injuries to the SDFT are represented by the same level of deterioration or structural change, so there is not a one-size-fits-all pathology or diagnosis, and therefore there cannot be a cure-all treatment.
Most tendon injuries have a sneaky onset with tendon degeneration developing initially without clinical signs, so problems start without you or your horse even knowing about them. Often by the time you realize there is a problem, tendon matrix degradation has already begun.
Staging the structural integrity of the tendon or classifying the extent of structural deterioration present is, therefore, imperative—not only for optimal therapy selection and appropriate rehabilitation guidance but also if prevention of injury is ever to be achieved.
Why isn’t conventional ultrasound enough?
Unfortunately, although conventional ultrasound has historically been used to evaluate equine tendon, limitations have restricted its ability to accurately monitor tendon structure, predict injury or guide rehabilitation.
Clinical improvement is usually not accurately correlated with changes in imaging status using conventional ultrasound, especially in the later stages of healing with conventional ultrasound not demonstrating enough sensitivity to determine the type of tendon tissue under investigation.
So, while regular ultrasound can easily demonstrate the presence of a core lesion when it first appears, by about two months post injury, its capacity to provide information regarding the health of the tendon is limited. Because of its inability to interpret the integrity of the underlying tendon structure accurately, along with inconsistencies in imaging, reliance on operator skills and the inherent lack of ability of a 2D conventional ultrasound image to fully decipher a 3D tendon structure, its ability to reliably evaluate and monitor the SDFT following the initial acute period is severely restricted.
What is ultrasound tissue characterisation?
Ultrasound tissue characterisation is a relatively new technique intended to alleviate some of the problems encountered with conventional ultrasound by improving objective tendon characterisation. It does this by providing a 3D reconstruction of the tendon and by classifying and then quantifying tendon tissue into one of four colour-coded echo types based on the integrity of the tendon structure.
It can assess in detail the structural integrity of the tendon; it can discriminate a variety of pathological states and is sensitive enough to detect the effect of changing loads on the tendon within days.

Figure 2: Color-coded ultrasound tissue characterization echo types represent the stability of echo pattern over contiguous images related to tendon matrix integrity.
What do the colors mean? (Figure 2)
Green (type 1 echoes) are normal, well-aligned and organized tendon bundles, and at least 85-90% of this echo type should be found in a healthy tendon (SDFT). Blue (type 2 echoes) are areas of wavy or swollen tendon bundles. They can represent remodeling and adapting tendon or inferior repair. Red (type 3 echoes) represents fibrillar tissue (the smaller basic unit or building block of tendon). This echo type can represent partial rupture of the tendon where they reflect breakdown of normal structure or they can represent initial healing as the tendon begins to rebuild. Black (type 4 echoes) are areas of cells or fluid and represent core lesions where no normal tendon tissue exists.
How is ultrasound tissue characterization currently used?
The aim of ultrasound tissue characterization is not to replace conventional ultrasound but on the contrary, it is recommended to perform an evaluation with both conventional B mode ultrasound and ultrasound tissue characterization to achieve a complete picture of tendon health.

Figure 3: Ultrasound tissue characterization tracker frame with attached ultrasound probe.
Currently it is used successfully in elite human athletes such as NBA and soccer players to monitor the health of their tendons (Achilles tendon and patellar tendons) and to guide exercise regimens post injury.
In the equine field, it is used in elite sport horses as part of routine maintenance evaluations to direct exercise, to monitor tendon health and guide rehabilitation following an injury.
How does it work?
It consists of a standard linear ultrasound probe mounted onto a motorized tracking device (Figure 3). Due to the sensitivity of this equipment, the limbs should be clipped in order to obtain good quality images.
The probe moves non-invasively and automatically down the tendon from top to bottom over a 12-cm scanning distance (see Introphoto) …



BUY THIS ISSUE IN PRINT OR DOWNLOAD
4 x print issue and online subscription to European Trainer & online North American Trainer. Access to all digital back issues of both editions.
Your subscription will start with the October - December 2025 issue - published at the end of September.
If you wish to receive a copy of the most recent issue, please select this as an additional order.
Gerald Leigh Memorial Lectures 2020 - minimising risk from equine infectious disease - how it will hopefully help support education on equine infectious disease
By Celia M Marr
IN ASSOCIATION WITH:

COVID-19 has affected all corners of the thoroughbred world and has changed lives, work patterns and the social activity that underpins racing. One of its minor impacts was that this year, the Gerald Leigh Memorial Lecture series, usually coordinated by Beaufort Cottage Educational Trust at the National Horseracing Museum, Palace House, Newmarket each summer, was cancelled.
This annual lecture series is supported by the Gerald Leigh Charitable Trust in honour of Mr Leigh’s passion for the thoroughbred horse and its health and welfare. Coincidentally, the topic which had been selected for 2020 was Minimising Risk from Equine Infectious Disease. Finding that a meeting was impossible, the trustees organised for presentations to be filmed remotely, and these are now available online.

THE LECTURES SERIES INTRODUCTION BY NICK WINGFIELD DIGBY, CHAIRMAN, BEAUFORT COTTAGE TRUST
Gastrointestinal disease is a common problem in foals and youngstock with potentially serious illnesses involved. Dr Nathan Slovis, director of the McGee Center, Lexington, Kentucky, USA, explained that by six months of age, 20% of foals will have had infectious diarrhoea. Dr Slovis presents a concise and very practical account of how we can minimise risk of infection in this age group.
The specific causes of gastrointestinal disease vary with age. Foals frequently display mild diarrhoea at around the time of the foal heat, generally a problem that will clear up uneventfully. Major infections in foals include rotavirus, Salmonella, Clostridium perfringens, Clostridium difficile. Infectious disease can be life-threatening if infection leads to shock, so every gastrointestinal case should be assessed carefully; early intervention is critical.
Vaccines are available to help minimise risk of rotavirus but prevention relies primarily on proper hygiene and appropriate choice of disinfectants, which vary depending on the particular microorganism concerned.

PRESENTATION BY DR NATHAN SLOVIS, DIRECTOR OF THE MCGEE CENTER, LEXINGTON, KENTUCKY
Diagnosis: PCR and ELISA technologies
The speed and availability of laboratory testing have been revolutionised in recent years with the introduction of ELISA and PCR technology. The enzyme-linked immunosorbent assay (ELISA) is an immunological assay commonly used to measure antibodies, antigens or proteins. An ELISA test relies on finding a molecule which is unique to a virus or bacteria and is used to find several equine pathogens, including rotavirus, Clostridium difficile and Clostridium perfringens.
PCR technology rapidly makes millions to billions of copies of a specific DNA sample, allowing the lab to take a very small sample of DNA and amplify it to a large enough amount to study in detail. Rapid tests are now available, which have revolutionised the diagnostic approach across a huge range of equine infections; relevant to foal diarrhoea is that this technology is used for rapid testing of faecal samples for Salmonella.
In addition to being extremely quick, both PCR and ELISA tests are very sensitive. Dr Slovis emphasised how important this is in early identification of diseases with the potential to spread rapidly in young horses.
Auditing environmental contamination
All the speakers in the webinar series spoke of the importance of robust biosecurity and common themes emerged in all four webinars regardless of the animals’ age or whether respiratory, skin or gastrointestinal infection is involved.
Dr Slovis’ clinical practice includes offering services to identify areas of environmental contamination. This involves a detailed inspection of all areas on the farm together with laboratory testing for the common pathogens. Key benefits of a facility evaluation service are to help support staff education and to highlight areas of weakness in biosecurity practices; and farmers and vets can work together to devise practical solutions to farm-specific problems. In his webinar, Dr Slovis shows some great examples of what not to do, which are drawn from his extensive experience of advising on biosecurity practices in equine facilities.

THE PRESENTATION BY PETER RAMZAN, A MEMBER OF THE RACING TEAM AT ROSSDALES LLP, NEWMARKET, UK:
Infectious challenges in young horses on training yards
Peter Ramzan, member of the Racing Team at Rossdales LLP, Newmarket discussed how to reduce risks when horses move into training. Piet is a fellow of the Royal College of Veterinary Surgeons and has written extensively on a range of disorders affecting horses in training. He summarised three areas relevant to this age group: lower respiratory tract disease, ringworm and the rare but sporadic disease threats such as strangles and neurological herpes.
Lower respiratory tract disease
This problem is mainly responsible for coughing and affects around 80% of two-year-olds and 25% of three-year-olds. Research in Newmarket has shown that for every 100 horses, there are around 10 cases each month, but prevalence varies between yards and seasons with a peak in early spring. Bacteria are believed to be a more common cause than viral infection, but both can cause coughing and can occur simultaneously.
Prevention is better than cure
Exposure to disease-causing microorganisms is inevitable and cannot be prevented, but risk of clinical disease can be reduced by optimising immunity. It is helpful if exposure occurs prior to or early in training. Ramzan concluded that homebreds that have bypassed public sales and the inevitable mixing with other horses there are at greater risk of interruptions to their training when they do enter yards as two-year-olds. He went on to emphasise that it is not necessarily helpful to aggressively treat respiratory infections in pre-training—better to let infection run through yearlings and young two-year-olds, providing that they remain mildly affected as this helps them build immunity to protect them during their racing careers.
As well as discussing the biosecurity measures which apply across all age groups and disease threats, particular points that Ramzan emphasised for reducing the impact of infectious disease in training yards included the importance of avoiding the introduction of yearlings to the main yards before the end of the season and adoption of a strategic vaccination programme. Vaccines should be given to horses in a year ahead of the influx of yearlings while maintaining immunity throughout the racing season; autumn and spring boosters are most likely to achieve this.
Antimicrobial stewardship
It is increasingly clear that overuse of antimicrobials is promoting resistance to these potentially lifesaving drugs. Vets and trainers should avoid their use, except where bacterial infection is highly likely, or ideally confirmed with laboratory testing. Ideally the lowest class of antibiotics should be used first, reserving protected classes, such as enrofloxacin and ceftiofur. Ramzan shared data from his practice over the last two decades which showed an alarming increase in resistance to oxytetracycline, which is the commonly used antimicrobial. Conversely, in the same period, oral trimethoprim sulphonamide, which is not used as much as it could be, has had a rise in sensitivity, likely because it is not used as often as it could be.
Herpes virus Type 1: a uniquely challenging foe
Professor Lutz Goehring, head of Equine Medicine and Reproduction at Ludwig-Maximilian University, in Munich, Germany, has had a distinguished research career focussed on equine herpes type 1 (EHV1). This virus has the potential to cause both abortion storms and outbreaks of neurological disease in all age groups, including horses in training.

PRESENTATION BY PROF. LUTZ GOEHRING IS HEAD OF EQUINE MEDICINE AND REPRODUCTION AT LUDWIG-MAXIMILIAN UNIVERSITY, IN MUNICH, GERMANY.
Equine Herpes Virus is a real threat to horse health and performance. Racing yards can be particularly vulnerable to outbreaks, but there are some easy steps you can take to reduce the risks.
Dr Wendy Talbot, vet at Zoetis explains: EHV is a contagious viral infection causing respiratory disease, abortions and neurological disease. Carrier horses show no clinical signs, but the virus can be reactivated at any time and spread to other horses and this is more likely to happen during times of stress. 1,2,3
EHV can be transmitted by direct horse-to-horse contact and by nasal or ocular discharge, which can spray or travel through the air over short distances. It can also be spread by sharing infected equipment, and via people who have been in contact with infected horses. This is why it’s crucial to have good biosecurity measures in place at yards, races, training and sales events. 4
Signs of the virus can be visually obvious or very subtle: horses may have a nasal discharge, weepy eyes, swollen glands and a cough and fever or a less noticeable lethargy, lack of appetite and reduced performance. 1,5
Vaccination against EHV is important because it helps tip the balance in favour of the horse’s immune system and reduces viral shedding.
Vaccination programmes should run concurrently with rigorous hygiene and isolation protocols to help minimise the risks of EHV spreading.
It’s also important not to mix unvaccinated horses with vaccinated ones to provide the best level of protection. 6,7
If you think any of your horses may have any symptoms of respiratory disease,isolate them immediately and contact your vet to discuss the next course of action.
FOR FURTHER INFORMATION FOLLOW THIS LINK
1. Slater J (2014) Equine Herpesviruses. In: Equine Infectious Diseases. Eds., D.C. Sellon and M. Long, Saunders, St. Louis. P151-169
2. Allen GP (2002) Respiratory Infections by Equine Herpes Virus Types 1 and 4. International Veterinary Information Service.
3. Slater J. What is Equine Herpes Virus? Accessed August 2019 https://www.horsedialog.co.uk/Health/WhatisEHV.aspx
4. Allen, GP (2002) Epidemic disease caused by equine herpesvirus-1: recommendations for prevention and control. Equine Veterinary Education; 14(3):136-142.
5. Davis, E. (2018) Disorders of the respiratory system. In: Reed SM, Bayly WM, Sellon DC, eds. Equine Internal Medicine, 4th ed. St Louis, MO: Elsevier:313-386.
6. Lunn, DP., et al. (2009) Equine herpesvirus-1 consensus statement..J Vet Intern Med. 23(3). 450-461
7. Equine herpesviruses: a roundtable discussion Philip Ivens, David Rendle, Julia Kydd, James Crabtree, Sarah Moore, Huw Neal, Simon Knapp, Neil Bryant J Richard Newton Published Online:12 Jul 2019 https://doi.org/10.12968/ukve.2019.3.S2.1
EHV1, like its virus relatives that cause cold sores in humans, has the ability to become latent. This means that the virus can sit in an inactive form in certain nerves and lymph node tissues, only to be reactivated and start to spread amongst groups of horses. While latent, the virus is out of reach of the immune system. Latent infection with EHV1 is widespread in horse populations globally.
Reactivation of EHV1 is not a common event, but it is associated with “stressful” situations such as mixing with new horses, transport, above-normal exercise, and in mares with foaling. Understanding the mechanisms involved in reactivation, spread to other horses and subsequent uptake of the virus into tissues—such as the placenta and fetus to cause abortion and to the spinal cord to cause neurological signs and paralysis—has been the main focus of Prof Goehring’s research career.
EHV1 is easy to kill with soaps and disinfectants when it is outside the body, again highlighting the importance of good biosecurity practices in studs and training yards. The virus spreads from horse to horse when there is close contact and droplets breathed out by an infected horse are inhaled by another. Shortly after inhaling the virus, there is a short temperature spike and then a second more intense spike usually occurs 8-10 days later. Neurological signs or abortion will typically come days or weeks after this second temperature spike.
Outbreak mitigation
Early detection and effective quarantine are the mainstays of EHV1 outbreak prevention. In the face of a potential outbreak, swift action to stop spread is critical. Movement on and off the property must cease. Horses with subtle clinical signs—slight nasal discharge, lymph node enlargement and fever—can now be tested very quickly for EHV1 using a nasal swab PCR. Horses should be tested to identify any that are shedding the virus; and any which are positive must be removed to isolation. Horses housed near these individuals should be quarantined in case they are incubating the disease. Horses in the early stages of infection may benefit from treatment to prevent neurological complications.
Distance is the key to stopping this droplet-aerosol infection; and although the distance does not need to be great, more is always better. Traditionally racehorses exercise in strings. An exercising horse which is shedding virus creates a tail of viral particles trailing behind it. In his webinar, Prof Goehring talked about the advantages of increasing distance between exercising horses and showed the benefits of exercising alongside rather than one behind the other. When there is infection around, consideration should also be given to the order horses go out to exercise, with those least likely to have infection exercising first.
Immunity, current and future vaccines
Following infection or vaccination, horses produce both antibodies and specialised cells with the ability to fight off EHV1 infection. Vaccination can be expected to reduce both the clinical signs and the shedding of virus if they are challenged. However, this immunity gradually wanes with time and with currently available herpes virus vaccines, repeat vaccination every six months is recommended
.
It is also important to understand that there is a balance between immunity level and infectious dose such that horses which are challenged with a very high dose of virus are more likely to develop fever than those that are exposed to a low dose—this again highlights the importance of effective biosecurity practices on studs and training yards.
Finally, although not yet available for equine herpes viruses, novel sub-unit vaccines introduced for similar herpes viruses in humans have been shown to cement latent virus into its hidden location and stop reactivation. Prof Goehring suggested this technology may be the light at the end of the tunnel for horses because this novel approach may reduce the likelihood of the outbreak initiation, which begins with reactivation of latent virus.

PRESENTATION OF DR. RICHARD NEWTON, DIRECTOR OF EPIDEMIOLOGY AND DISEASE CONTROL AT THE ANIMAL HEALTH TRUST, KENTFORD, UK.
Lessons from the European flu epizootic 2019
Although current attention is on COVID-19, it is important to reflect on lessons from the equine influenza outbreak which affected many countries in Europe last year. Dr Richard Newton, epidemiologist and an authority on equine infectious disease, coordinated much of the UK’s surveillance and communication during this outbreak, working at that time at the Animal Health Trust, Newmarket, Suffolk.
Equine influenza is a contagious rapidly-spreading viral respiratory disease. Common signs of infection include fever and coughing; and coughing is an important factor in spread as infected particles are released and can spread over wide distances to affect others. Unlike EHV1, there is no carrier or latent state, and the flu virus needs chains of transmission to persist in a horse population; an infected horse has to pass the virus on to another in order for the infection to perpetuate in a group. Vaccination is used to break these chains of transmission by reducing susceptibility. However, flu virus evolves continuously, constantly producing new strains; and in order to be effective, vaccine strains must keep up with this evolution and be updated periodically.
The R number: what does it mean?
The R number, or basic reproduction number, is the number of cases on average that one case generates over the course of its infectious period. If the R number is less than one, the chain of transmission will die out, and infection will cease. Vaccination plays a major role in reducing the R number by limiting the number of susceptible animals.
Lessons from 2019
Flu occurred in several countries in Europe last year. In the UK, we saw two waves of this infection whereas other countries, notably Ireland and Holland, had different patterns. The Clade 1 strain of virus involved in the 2019 outbreak had not been seen in Europe for over a decade.
Flu mainly affects non-vaccinated horses but can occur in vaccinated animals, particularly if a new strain challenges a population. Fortunately, prompt action by the British Horseracing Authority last year minimised flu occurrence within our racing population. In January, based on information coming out of other European countries, the BHA veterinary committee advised six monthly booster vaccinations.
A six-day stoppage in racing and horse movements after flu was identified in a racing yard in early February. The majority of flu outbreaks occurred in unvaccinated horses, and the second spike seen in the summer of 2019, was associated with horse gatherings at shows and fairs. Nevertheless 18% of flu cases involved appropriately vaccinated animals, some of which might have been vaccinated after contracting infection, while many of the others were nearing the time when a booster was due.
The UK’s racing populations are highlight connected, and the racing stoppage was prompted by the occurrence of flu in vaccinated animals. This break provided the necessary pause during which the scale of infection could be assessed. A huge number of racehorses were tested, and Dr Newton explained that an important conclusion from this experience was that there is a need to scale up lab testing capacity to support such a response in future, particularly if we were to be challenged by a completely novel strain of flu.
What did we do well?
Racing heeded the earliest warnings with its six-month booster recommendation, applied a lockdown and implemented test and trace and finally, on releasing lockdown, racing applied biosecurity precautions, concepts now familiar to us all in relation to COVID-19.
Dr Newton acknowledged that these lessons were missed or ignored outside of racing, leading to a second wave in the non-thoroughbred during the summer; and horse owners and event organisers did not adequately embrace the simple messages regarding the importance of vaccination and isolation. Many of the outbreaks which occurred last summer were associated with the introduction of new animals on a premise. The UK horse population has a low national vaccine coverage, estimated at around 40%—a statistic which puts the UK in a poor light compared to other European countries where uptake in the general horse population is much higher.
Do we need to improve vaccines and vaccine strategy?
Vaccine strains are continuously reviewed by The World Organisation for Animal Health (OIE) panel—critical work which in the UK is supported by the Horserace Betting Levy Board. Currently there is insufficient scientific evidence to recommend an equine influenza vaccine strain update, although this might not be far away. On the other hand, reducing booster vaccine intervals is clearly beneficial. Flu vaccines work by stimulating the horse to produce antibodies which decline with time. There is variation in vaccine response between individual horses with some animals less well protected than others. Dr Newton reviewed information from multiple studies and outbreaks and concluded the weight of evidence overwhelmingly supports a six-monthly booster. Increasing vaccine uptake across the national herd will involve improved education in the non-thoroughbred world but is critical to supporting herd immunity. Improved awareness will benefit all horses including thoroughbreds.
Take-home messages
All four speakers highlighted practical biosecurity measures as critical in reducing the risks of infectious disease. Vaccines are essential for both flu and EHV1. They are not infallible, and ongoing research will lead to improved vaccine technology. Most important of all is that education of people working with thoroughbreds, and across the wider equestrian world, will help support early recognition and management of disease when it occurs. This year’s Gerald Leigh Memorial Lectures will hopefully help support this education by making information on equine infectious disease available online.


BUY THIS ISSUE IN PRINT OR DOWNLOAD
4 x print issue and online subscription to European Trainer & online North American Trainer. Access to all digital back issues of both editions.
Your subscription will start with the October - December 2025 issue - published at the end of September.
If you wish to receive a copy of the most recent issue, please select this as an additional order.
Minimising serious fractures of the racehorse fetlock - risk reducing of catastrophic fractures associated with the fetlock joint

By VA Colgate, PHL Ramzan & CM Marr
Minimising serious fractures of the racehorse fetlock
In March 2020, a symposium was held in Newmarket, UK, aiming to devise measures which could be used internationally to reduce the risk of catastrophic fracture associated with the fetlock joint. The meeting was supported by the Gerald Leigh Charitable Trust, the Beaufort Cottage Charitable Trust and the Jockey Club with additional contributions from a number of industry stakeholders. On the first day a panel of international experts made up of academic professors, Chris Whitton (Melbourne, Australia), Sue Stover (Davis, California), Chris Kawcak (Colorado), Tim Parkin (Glasgow) and Peter Muir (Wisconsin); experienced racehorse clinicians, Ryan Carpenter (Santa Anita) and Peter Ramzan (Newmarket); imaging experts, Sarah Powell (Newmarket) and Mathieu Spriet (Davis, California); and vets with experience in racing regulatory bodies, Scott Palmer (New York) and Chris Riggs (Hong Kong) joined forces to discuss risk assessment protocols, particularly those based on imaging features which might indicate increased risk of imminent fracture. This was followed by a wider discussion with a diverse invited audience of veterinary and industry stakeholders on how our current knowledge of fracture pathophysiology and risk factors for injury could be used to target risk assessment protocols. A report of the workshop outcomes was recently published in Equine Veterinary Journal.
The importance of risk reduction
With the ethics of the racing industry now in the public spotlight, there is recognition that together veterinary and horseracing professionals must strive to realise an improvement in equine injury rates. Intervention through risk profiling programmes, primarily based on training and racing metrics, has a proven track record; and the success of a racing risk management program in New York gives evidence that intervention can and will be successful.
The fetlock of the thoroughbred racehorse is subjected to very great loads during fast work and racing, and over the course of a training career this can result in cumulative changes in the bone underlying the articular cartilage (‘subchondral’ bone) that causes lameness and may in some circumstances lead to fracture. Fracture propagation involving the bones of the fetlock (cannon, pastern or proximal sesamoid bones) during fast work or racing can have catastrophic consequences, and while serious musculoskeletal injuries are a rare event when measured against race starts, there are obviously welfare and public interest imperatives to reduce the risk to racehorses even further. The dilemma that faces researchers and clinicians is that ‘fatigue’ injuries of the subchondral bone at some sites within the fetlock can be tolerated by many racehorses in training while others develop pathology that tips over into serious fracture. Differentiating horses at imminent risk of raceday fracture from those that are ‘safe’ to run has not proven particularly easy based on clinical grounds to date, and advances in diagnostic imaging offer great promise.
Profiling to inform risk assessment
Risk profiling examines the nature and levels of threat faced by an individual and seeks to define the likelihood of adverse events occurring. Catastrophic fracture is usually the end result of repetitive loading, but currently there are no techniques that can accurately determine that a bone is becoming fatigued until some degree of structural failure has actually occurred. However, diagnostic imaging has clear potential to provide information about pathological changes which indicate the early stages of structural damage.
Previous research has identified a plethora of epidemiological factors associated with increased risk of serious catastrophic musculoskeletal injury on the racetrack. These can be distilled into race, horse and management-related risk factors that could be combined in statistical models to enable identification of individual horses that may be at increased risk of injury.
In North America, the Equine Injury Database compiles fatal and non-fatal injury information for thoroughbred racing in North America. Since 2009, equine fatalities are down 23%; and important risk factors for injury have been identified, and this work has driven ongoing improvement.
The problem with all statistics-based models created so far for prediction of racehorse injury is that they have limited predictive ability due to the low prevalence of racetrack catastrophic events. If an event is very rare, and a predictive tool is not entirely accurate, many horses will be incorrectly flagged up as at increased risk. At the Newmarket Fetlock workshop, Prof Tim Parkin shared his work on a model which was based on data from over 2 million race starts and almost 4 million workout starts. Despite the large amount of data used to formulate the model, Tim Parkin suggested that if we had to choose between two horses starting in a race, this model would only correctly identify the horse about to sustain a fracture 65% of the time. Furthermore, the low prevalence of catastrophic injury means it will always be difficult to predict, regardless of which diagnostic procedure is employed.
Where do the solutions lie?

A radiograph showing a racing thoroughbred’s fetlock joint. The arrow points to a linear radiolucency in the parasagittal groove of the lower cannon bone—a finding that is frequently detectable before progression to serious injury.
One possible strategy to overcome the inherent challenge of predicting a rare event involves serial testing. Essentially with this approach, a sequence of tests is carried out to refine sub-populations of interest and thus improve the predictive ability of the specific tests applied. An additional consideration in the design of any such practical profiling system would have to be the ability to speedily come to a decision. For example, starting with a model based on racing and training metrics such as number of starts and length of lay-off periods, as well as information about the risk associated with any particular track or racing jurisdiction, entries could be screened to separate those that are not considered to be at increased risk of injury from a smaller sub-group of horses that warrant further evaluation and will progress to Phase 2. The second phase of screening would be something relatively simple. Although not yet available, there is hope that blood tests for bone biomarkers or genetic profiles could be used to further distil horses into a second sub-group. This second sub-group might then be subjected to more detailed veterinary examination, and from that a third sub-group, involving a very small and manageable number of horses flagged as potentially at increased risk, would undergo advanced imaging. The results of such diagnostic imaging would then allow vets to make evidence-based decisions on whether or not there is sufficient concern to prompt withdrawal of an individual from a specific race from a health and welfare perspective. Of course there are other considerations which limit the feasibility of such a system, including availability of diagnostic equipment and whether or not imaging can be quickly and safely performed without use of sedation or other drugs, which are prohibited near to a race start.
Diagnostic techniques for fetlock injury risk profiling
Currently there is no clear consensus on the interpretation of images from all diagnostic imaging modalities, and important areas of uncertainty exist. Although a range of imaging modalities are available, each has its own strengths and weaknesses, and advances in technology currently outstrip our accumulation of published evidence on which to base interpretation of the images obtained.
Interpretation is easy when the imaging modality shows an unequivocal fracture such as a short fissure in a cannon bone. Here the decision is simple: the horse has a fracture and must stop exercising. Many cases, however, demonstrate less clearly defined changes that may be associated with bone fatigue injury.
Currently radiography remains the most important imaging modality in fetlock bone risk assessment. With wide availability and the knowledge gained by more advanced imaging techniques refining the most appropriate projections to use; radiography represents a relatively untapped resource that through education of primary care vets could immediately have a profound impact on injury mitigation. The most suitable projection with which to detect prodromal condylar fracture pathology in the equine distal limb is the flexed dorsopalmar (forelimb) or plantarodorsal (hindlimb) projection. On this projection, focal radiolucency in the parasagittal groove, whether well or poorly defined, with or without increased radio-opacity in the surrounding bone, should be considered representative of fracture pathology unless evidence from other diagnostic imaging modalities demonstrates otherwise.
Computed Tomography (CT) excels at identification of structural changes and is better than radiography at showing very small fissures in the bone. However, additional research is needed to determine specific criteria for interpretation of the significance of small lesions in the parasagittal groove with respect to imminent risk of serious injury. There are good indications that fissure lesion size and proximal sesamoid bone volumetric measurements have the potential to be useful criteria for prediction of condylar and proximal sesamoid bone fractures respectively. With technological advancement, it is likely that CT will be more widely used in quantitative risk analysis in the future.
Magnetic Resonance Imaging (MRI) has the ability to detect alterations in the fluid content of bones, which allows assessment of acute, active changes. Indeed standing, low-field MRI has been shown to be capable of detecting bone abnormalities not readily identifiable on radiography and has been successfully used for injury mitigation in racehorse practice for some time. However, when used for evaluation of cartilage and subchondral bone lesions, there is a relatively high likelihood of false positive results.

PET is the most recent advance in diagnostic imaging. It is being developed in California and, when combined with CT, provides information on bone activity and structure. In these three images of the same fetlock, from different aspects, the orange spots indicate increased activity in the proximal sesamoid bone, which is a potential precursor to more serious injury.
Image courtesy of Dr M. Spriet, University of California, Davis.


BUY THIS ISSUE IN PRINT OR DOWNLOAD
The differences between a healthy/unhealthy biome - gastrointestinal disease - disturbances of the gut bacteria

By Carol Hughes
Gastrointestinal diseases and upsets are common in thoroughbred racehorses, causing discomfort, loss of performance and even mortality. Every common gastrointestinal disease can be linked back to disturbances (dysbiosis) of the gut bacteria. Currently, new gene technology is driving research at an intense rate, providing new insights into the equine microbial community (1) and providing both trainer and the vet with a powerful and accurate analytical tool to improve health and manage disease.
The gastrointestinal tract of the horse is colonized by trillions of microorganisms, which includes 1,000-1,500 different species, making up around 95% of the biome; the other 5% are made up of archaea, protozoa, fungi and viruses. Though most studies concentrate on identifying species of bacteria and linking to health and disease. Other members of the biome have equally important roles to play. In the racehorse, a major player is the Enterobacteria phage PhiX174, which is a bacterial virus that protects the horse against E-coli (2).
The microbial community has co-evolved with the host, performing essential and vital activities such as the extraction of energy and nutrients from foodstuff, synthesis of vitamins, interaction with the immune system and cross talk with the brain, which is thought to affect temperament and behaviour. Taxonomic and functional compositions of the gut microbiome are rapidly becoming viable indicators of horse health and disease.
Each member of the microbial community has a different but synergistic role, which is beneficial to the health of the horse; e.g., the fungi break down the indigestible parts of forage plants, such as the polysaccharides, whilst the ciliate protozoa contribute to the process by producing a wide range of enzymes that the horse is unable to make, impacting and benefitting the immune system. Microbial fermentation of cellulose, hemicellulose and lignin reduces the structural and non-structural plant wall material into carbohydrates, proteins (amino acids) and lipids, and produces volatile and short chain fatty acids (2a), which are the primary source of energy for the horse. The bacteria contribute the most to the degradation of ingested food, producing the final components of the fermentation process, which are acetic, propionic and butyric acid, methane and carbon dioxide.
The gastrointestinal tract of the horse is sensitive to change, stress, environment and medication, which cause imbalances or dysbiosis (3). Establishing or profiling a healthy baseline in the horse is difficult as variations exist between individuals, breeds, diets and locations; the thoroughbred racehorse is a very different animal to the Shetland pony or an Irish Draught. Fitness training alters the microbiome further; for these reasons it is important to study the thoroughbred as a population separate from other breeds and to analyse, where possible, racehorses training in a similar environment and location.
With this in mind, since 2017 there has been an ongoing project to study and profile the microbial populations of over 1,000 racehorses based in Newmarket, throughout the racing season; and the data produced has been used to develop profiles of the differences between a healthy/unhealthy biome. The project utilizes the cutting-edge Illumina MiSeq technology, which is the most accurate and up-to-date, preferred by genomic researchers around the world.
The Biome In Health
Elite racehorses have higher levels of a super-phylum bacteria
Questions asked….
Elite racehorses are trained to achieve peak fitness, but is it possible that they can gain an extra edge from the input of the hind gut bacteria?
How different is the microbiome of a Group 1 horse, and is it possible to identify the bacteria responsible for the extra edge?
Answers found….
Human scientists have known for some time that the microbiome of an elite human athlete is different (4), with faster metabolic pathways (amino acids and carbohydrates) and higher levels of faecal metabolites (microbial-produced short-chain fatty acids) acetate, propionate and butyrate associated with enhanced muscle fitness. The human and elite equine athlete do share similar microbial profiles, having higher percentages of the bacteria that manufacture short-chain fatty acids and higher levels of the super-phylum verrucomicrobia; these increase as the season/training progresses.

Image of the analysis of the microbiome of a Group 1 horse, compared to a non- group horse.
What is known about this super-phylum?
It has two main members: Methylacidiphilaceae and Akkermansia
Verrucomicrobia Methylacidiphilaceae thrive and proliferate on the ammonia produced from the degradation of starch and protein (5), whereas starch produces very high levels of ammonia. The bacteria make enzymes (ammonia monooxygenase) (6), which convert ammonia into nitric oxide (7). The nitric oxide has three major benefits to a racehorse:
Helps repair and renew the gut wall (8)
Enhances performance and increases exercise tolerance (9)
Improves vascular function and metabolism (10)
Verrucomicrobia Akkermansia is a mucus-eating specialist, living and thriving within the gut wall, digesting mucin from the mucosal lining (10a) with a unique ability to metabolise galactose and melibiose (11) for energy. Akkermansia in the human biome significantly increases the numbers of metabolic pathways. Horses with gastric ulcers have very low levels, perhaps indicating its function in both performance and disease.
Comparing percentages of the super-phylum amongst other breeds/locations/environments gave good insight into how important and relevant verrucomicrobia is to the racehorse.
Verrucomicrobia varied significantly from group to group; the lowest levels were found in the sedentary and/or companion animal group which was comprised of 250 horses (gently hacked or unridden companions). The Carneddau are an ancient herd of wild horses that graze freely in the mountains of Snowdonia, and the Pottokas are from Spain. The CCI-L group was made up of 10 horses eventing at International One Day Event Level.
The Non-Group horses were based in Newmarket and analysed at the height of the flat season in July, whilst the Group 1 horses started the season (Feb) with levels of 10%; these levels increased as the season continued until finally levelling out at 23% in July through to September when the testing finished.

Fig 3: The microbiome of Group 1 horses indicating higher diversity and stability.
Fig 4: Image of thoroughbreds in training diagnosed with EGGD.
Why the horses diagnosed with Equine Glandular Gastric Disease had lower levels of verrucomicrobia is unknown at this time, horses with EGGD had a completely different profile to the healthy Group 1 horses. See Fig 3 and 4. …


BUY THIS ISSUE IN PRINT OR DOWNLOAD
Radiofrequency therapy - used for reducing pain - managing inflammation - aiding tissue repair - reducing muscle spasm

By Helen Walsh, BSc, MCSP, HCPC
It’s the phone call guaranteed to chill any trainer’s blood in the days after a win: ‘A prohibited substance has been detected; your horse has been disqualified’.
It’s a devastating blow. The reward for all the blood, sweat and tears leading up to a race win is snatched away to be replaced by questions, namely ‘how’ and ‘when’?

Any Currency ‘winning’ the Glenfarclas Cross Country Chase, 2016.
This nightmare scenario happened to trainer Martin Keighley back in 2016 at the Cheltenham Festival with Any Currency in the Glenfarclas Cross Country Chase. After a brilliant win and much celebration, a test revealed traces of triamcinolone acetonide (TCA), a synthetic cortisone. It’s one that can legally be used in training for appropriate conditions, which it had been, but must not be present on race day. The British Horseracing Authority (BHA) refuses to give advice regarding detection times for intra-articular injections as there isn’t enough data to determine an exact time; and there are lots of variants that could lengthen the duration it can be detected in the body.
Any Currency had been given the injection 42 days before competing. This is a substantial amount of time, and no one would have thought it would still be present in the horse’s system. Keighley was cleared of any wrongdoing, but the win—his first Festival victory—wasn’t reinstated.
This experience made Keighley even more cautious about using medication; he swore that this situation would not happen again. He already had animal physiotherapists working on his yard, providing regular performance maintenance and rehabilitation for the horses. As much as possible, medication was being avoided.
It was in September 2019 when one of his veterinary animal physiotherapists, Hannah Ashton, had arranged a lecture on electro-physical agents in tissue repair with the world-renowned Professor Tim Watson. During this lecture, research was presented on radiofrequency (RF). Far from it being just another electrotherapy fad, Prof Watson presented published lab work and clinical data using radiofrequency 448kHz as a direct current on the human body.

Trainer Martin Keighley with Lord Condi.
Hannah discussed this with Martin Keighley and the yard’s vet; having always been a great advocate of equine welfare, Keighley was keen to see if this could help in the treatment of injured horses but also prevent injury in the first place. They began a trial with the technology for three weeks and were amazed by the results; the tech became part of the horse’s ongoing maintenance and for rehabilitation when indicated following injury. Looking back at their data, they have seen a dramatic reduction in medication and reduced vet call outs; the horse’s wellbeing has improved with this addition to an already exceptional care package.
He isn’t the only one embracing this technology, having been widely used by Premier League football clubs for several years and been spotted in the videos posted via social media by cyclist Chris Froome of Team Ineos, and in national press with pro tennis player Rafael Nadal. It is delivered in their recovery, pre-training and before competition as well as when any injury occurs.
At this year’s Cheltenham Festival there were several successful horses who have received this treatment as part of their training and care plan in the lead-up to race day. Physiotherapist Polly Hutson mentioned her use of the technology in an interview with Radio 5 Live during day three of the Festival, right before two of the horses she treated finished second and first in the following races.

Hannah Ashton (Cotswold Horse & Hound Physiotherapy) treating one of Martin Keighley's 2020 season hopefuls.
So, what is radiofrequency in therapy?
It is an electromagnetic current operating at 448kHz that passes out of an active electrode and is in contact with the body; this current travels through the body to wherever the ‘return’ plate is located. The therapist can decrease the power so that nothing is felt, or increase it and the body will feel a warm sensation. It's relaxing when applied and is effective for reducing pain, managing inflammation, aiding tissue repair and reducing muscle spasm, to name a few.
Why is 448kHz important?
The technology has been researched at a cellular level by a bioelectrical magnetic team at University Hospital Ramon y Cajal in Madrid for over 21 years. They have published studies that show it's completely safe on the body at a cellular level. They have also published work on proliferation of stem cells and in greater detail, proliferation of cartilage cells. Their work has also explored differentiation of stem cells into their final cell type and on the specificity of radiofrequency signal on cancer cell death. This team refined the RF to 448kHz.
How does it work?
It’s a long answer but in simple terms, applying a current of this type directly to the body can have different effects. …


BUY THIS ISSUE IN PRINT OR DOWNLOAD
PET: the latest advance in equine imaging

By Mathieu Spriet, Associate Professor, University of California, Davis
Santa Anita Park, the iconic Southern California racetrack, currently under public and political pressure due to a high number of horse fatalities during the 2019 season, announced in December 2019 the installation of a PET scanner specifically designed to image horse legs. It is hoped that this one-of-a-kind scanner will provide information about bone changes in racehorses to help prevent catastrophic breakdowns.
What is PET?
PET stands for positron emission tomography. Although this advanced form of imaging only recently became available for horses, the principles behind PET imaging have been commonly used at racetracks for many years. PET is a nuclear medicine imaging technique, similar to scintigraphy, which is more commonly known as “bone scan”. For nuclear imaging techniques, a small dose of radioactive tracer is injected to the horse, and the location of the tracer is identified with a camera in order to create an image. The tracers used for racehorse imaging are molecules that will attach to sites on high bone turnover, which typically occurs in areas of bone subject to high stress. Both scintigraphic and PET scans detect “hot spots” that indicate—although a conventional X-ray might not show anything abnormal in a bone—there are microscopic changes that may develop into more severe injuries.
Development of PET in California
The big innovation with the PET scan is that it provides 3D information, whereas the traditional bone scan only acquires 2D images. The PET scan also has a higher spatial resolution, which means it is able to detect smaller changes and provide a better localisation of the abnormal sites. PET’s technological challenge is that to acquire the 3D data in horses, it is necessary to use a ring of detectors that fully encircles the leg.
The first ever equine PET scan was performed at the School of Veterinary Medicine at the University of California in 2015. At the time, a scanner designed to image the human brain was used (PiPET, Brain-Biosciences, Inc.). This scanner consists of a horizontal cylinder with an opening of 22cm in diameter. Although the dimensions are convenient to image the horse leg, the configuration required the horse be anesthetised in order to fit the equipment around the limb.

Figure 1: The first equine PET was performed in 2015 at the University of California Davis on a research horse laid down with anesthesia. The scanner used was a PET prototype designed for the human brain (piPET, Brain-Biosciences Inc., Rockville, MD, USA).
The initial studies performed on anesthetised horses with the original scanner demonstrated the value of the technique. A first study, published in Equine Veterinary Journal, demonstrated that PET showed damage in the equine navicular bone when all other imaging techniques, including bone scan, MRI and CT did not recognise any abnormality.

Figure 2: These are images from the first horse image with PET. From left to right, PET, CT, MRI and bone scan. The top row shows the left front foot that has a severe navicular bone injury. This is shown by the yellow area on the PET image and abnormalities are also seen with CT, MRI and bone scan. The bottom row is the right front foot from the same horse; the PET shows a small yellow area that indicates that the navicular bone is also abnormal. The other imaging techniques however did not recognize any abnormalities.
A pilot study looking at the racehorse fetlock, also published in Equine Veterinary Journal, showed that PET detects hot spots in areas known to be involved in catastrophic fractures. This confirmed the value of PET for racehorse imaging, but the requirement for anesthesia remained a major barrier to introducing the technology at the racetrack. To overcome this, LONGMILE Veterinary Imaging, a division of Brain-Biosciences Inc, in collaboration with the University of California Davis, designed a scanner which could image standing horses. To do this, the technology had to be adapted so that the ring of detectors could be opened and positioned around the limb.
With the support from the Grayson Jockey Club Research Foundation, the Southern California Equine Foundation and the Stronach Group, this unique scanner became a reality and, after the completion of an initial validation study in Davis, the scanner was installed at Santa Anita Park in December 2019.
PET at the racetrack….


BUY THIS ISSUE IN PRINT OR DOWNLOAD —
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Outlook for Stem Cell Therapy: its role in tendon regeneration

By Dr Debbie Guest
Tendon injuries occur very commonly in racing thoroughbreds and account for 46% of all limb injuries. The superficial digital flexor tendon (SDFT) is the most at risk of injury due to the large strains that are placed upon it at the gallop. Studies have reported that the SDFT experiences strains of up to 11-16% in a galloping a thoroughbred, which is very close to the 12-21% strain that causes the SDFT to completely rupture in a laboratory setting.

An acute tendon injury leads to rupture of the collagen fibres and total disruption of the well organised tendon tissue (Figure 1). There are three phases to tendon healing: an inflammatory phase that lasts for around one week, where new blood vessels bring in large numbers of inflammatory blood cells to the damaged site—a proliferative phase that lasts for a few weeks, where the tendon cells rapidly multiply and start making new collagen to replace the damaged tissue; and a remodelling phase that can last for many months, where the new collagen fibres are arranged into the correct alignment and the newly made structural components are re-organised.

Figure 1. A) The healthy tendon consists predominantly of collagen fibres (light pink), which are uniformly arranged with tendon cells (blue) evenly interspersed and relatively few blood vessels (arrows). B) After an injury the collagen fibres rupture, the tissue becomes much more vascular, promoting the arrival of inflammatory blood cells. The tendon cells themselves also multiply to start the process of rebuilding the damaged structure.
After a tendon injury occurs, horses need time off work with a period of box rest. Controlled exercise is then introduced, which is built up slowly to allow a very gradual return to work. This controlled exercise is an important element of the rehabilitation process, as evidence suggests that exposing the tendon to small amounts of strain has positive effects on the remodelling phase of tendon healing. However, depending on the severity of the initial injury, it can take up to a year before a horse can return to racing. Furthermore, when tendon injuries heal, they repair by forming scar tissue instead of regenerating the normal tendon tissue. Scar tissue does not have the same strength and elasticity as the original tendon tissue, and this makes the tendon susceptible to re-injury when the horse returns to work. The rate of re-injury depends on the extent of the initial injury and the competition level that the horse returns to, but re-injury rates of up to 67% have been reported in racing thoroughbreds. The long periods of rest and the high chance of re-injury therefore combine to make tendon injuries the most common veterinary reason for retirement in racehorses. New treatments for tendon injuries aim to reduce scar tissue formation and increase healthy tissue regeneration, thereby lowering the risk of horses having a re-injury and improving their chance of successfully returning to racing.
Over the past 15 years, the use of stem cells to improve tendon regeneration has been investigated. Stem cells are cells which have the remarkable ability to replicate themselves and turn into other cell types. Stem cells exist from the early stages of development all the way through to adulthood. In some tissues (e.g., skin), where cells are lost during regular turnover, stem cells have crucial roles in normal tissue maintenance. However, in most adult tissues, including the tendon, adult stem cells and the tendon cells themselves are not able to fully regenerate the tissue in response to an injury. In contrast, experimental studies have shown that injuries to fetal tissues including the tendon, are capable of undergoing total regeneration in the absence of any scarring. At the Animal Health Trust in Newmarket, we have an ongoing research project to identify the differences between adult and fetal tendon cells and this is beginning to shed light on why adult cells lead to tendon repair through scarring, but fetal cells can produce tendon regeneration. Understanding the processes involved in fetal tendon regeneration and adult tendon repair might enable new cell based and/or therapeutic treatments to be developed to improve tendon regeneration in adult horses.
In many tissues, including fat and bone marrow, there is a population of stem cells known as mesenchymal stem cells (MSCs). These cells can turn into cells such as bone, cartilage and tendon in the laboratory, suggesting that they might improve tendon tissue regeneration after an injury. MSC-based therapies are now widely available for the treatment of horse tendon injuries. However, research has demonstrated that after injection into the injured tendon, MSCs do not turn into tendon cells. Instead, MSCs produce factors to reduce inflammation and encourage better repair by the tissue’s own cells. So rather than being the builders of new tendon tissue, MSCs act as the foreman to direct tissue repair by other cell types. Although there is some positive data to support the clinical application of MSCs to treat tendon injuries in horses, placebo controlled clinical trial data is lacking. Currently, every horse is treated with its own MSCs. This involves taking a tissue biopsy (most often bone marrow or adipose tissue), growing the cells for 2-4 weeks in the laboratory and then injecting them into the site of injury. This means the horse must undergo an extra clinical procedure. There is inherent variation in the product, and the cells cannot be injected immediately after an injury when they may be the most beneficial.
To allow the prompt treatment of a tendon injury and to improve the ability to standardise the product, allogeneic cells must be used. This means isolating the cells from donor horses and using them to treat unrelated horses. Experimental and clinical studies in horses, mice and humans suggest that this is safe to do with MSCs, and recently an allogeneic MSC product was approved for use in the EU for the treatment of joint inflammation in horses. These cells are isolated from the circulating blood of disease-screened donor horses and are partially turned into cartilage cells in the laboratory. They are then available “off the shelf” to treat unrelated animals. Allogeneic MSC products for tendon injuries are not yet available, but this would provide a significant step forward as it would allow horses to be treated immediately following an injury. However, MSCs exhibit poor survival and retention in the injured tendon and improvements to their persistence in the injury site, and with a better understanding of how they aid tissue regeneration, they are required to enable better optimised therapies in the future.
Our research has previously derived stem cells from very early horse embryos (termed embryonic stem cells, ESCs. Figure 2). ESCs can grow in the laboratory indefinitely and turn into any cell type of the body. These properties make them exciting candidates to provide unlimited numbers of cells to treat a wide range of tissue injuries and diseases. Our experimental work in horses has shown that, in contrast to MSCs, ESCs demonstrate high survival rates in the injured tendon and successfully turn into tendon cells. This suggests that ESCs can directly contribute to tissue regeneration.

Figure 2. A) A day 7 horse embryo used for the isolation of ESCs. Embryos at this stage of development have reached the mare’s uterus and can be flushed out non-invasively. B) “Colonies” of ESCs can grow forever in the laboratory.
To understand if ESCs can be used to aid tendon regeneration, they must be shown to be both safe and effective. In a clinical setting, ESC-derived tendon cells would be implanted into horses that were unrelated to the original horse embryo from which the ESCs were derived. The recipient horse may therefore recognise the cells as “foreign” and raise an immune response against them. Using laboratory models, we have shown that ESCs which have been turned into tendon cells do not appear recognisable by the immune cells of unrelated horses. This may be due to the very early developmental stage that ESCs originate from, and it suggests that they would be safe to transplant into unrelated horses.
To determine if ESCs would be effective and improve tendon regeneration, without the use of experimental animals, we have established a laboratory system to make “artificial” 3D tendons (Figure 3).

Figure 3. Artificial 3D tendons grown in the laboratory are used to study different sources of tendon cells and help us work out how safe and effective an ESC-based therapy will be. A) Artificial 3D tendons are 1.5 cm in length. B) a highly magnified view of a section through an artificial tendon showing well-organised collagen fibres in green and tendon cells in blue.
ESC-tendon cells can produce artificial 3D tendons just as efficiently as adult and fetal cells, and this system allows us to make detailed comparisons between the different cell types.


BUY THIS ISSUE IN PRINT OR DOWNLOAD —
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Colic - effects of inflammation
By Dr Zofia Lisowski, Prof. Scott Pirie & Dr Neil Hudson
Overview of colic
Colic is a term used to describe the display of abdominal pain in the horse. It is the most common emergency in horses with four to ten out of every 100 horses likely to experience at least one episode of colic each year. It is also the single most common cause of equine mortality. In the US, one study showed that thoroughbreds were more likely to develop colic1 than other breeds. It is of great welfare concern to horse owners, and with the estimated costs associated with colic in the US exceeding $115 million dollars per year2 and the average cost of a horse undergoing colic surgery that requires a resection in the UK being £6437.803, it is also a significant economic issue for horse owners.
Horses with abdominal pain show a wide range of clinical signs, ranging from flank watching and pawing the ground in mild cases, to rolling and being unable to remain standing for any significant period of time in more severe cases. There are numerous (over 50) specific causes of colic. In general, colic occurs as a result of disruption to the normal function of the gastrointestinal tract. This may be attributable to mechanical causes such as an obstruction (constipation), distension (excess gas) or a volvulus (twisted gut). It may also have a functional cause, whereby the intestine doesn’t work as normal in the absence of an associated mechanical problem; for example, equine grass sickness is associated with a functional derangement of intestinal motility due to loss of nerves within the intestine.

Management of colic depends on the cause and can necessitate either a medical or surgical approach. Most horses with colic will either improve spontaneously or with simple medical treatment alone; however, a significant proportion may need more intensive medical treatment or surgery. Fortunately, due to improvements in surgical techniques and post-operative management, outcomes of colic surgery have improved over the past few decades with up to 85% of horses surviving to discharge. Crucially for the equine thoroughbred racehorse population, several studies focussed on racehorses that had undergone colic surgery and survived to discharge, reporting that 63-73% returned to racing. Furthermore, surgical treatment did not appear to negatively impact athletic performance. A similar finding was also seen in the general sport horse population.
Despite significant advancement in colic surgery per se, complications following surgery can have a significant impact on post-operative survival and return to athletic function. Common post-operative complications include:
Complications at the site of the incision (surgical wound)
Infection: Infections at the site of the surgical incision are relatively common. Antibiotics are usually administered before surgery and after surgery. Infections are not normally severe but can increase treatment costs. Horses that develop infections are at greater risk of developing an incisional hernia.
Hernia: Incisional hernias occur when the abdominal wall muscles fail to heal leaving a ‘gap’. Hernia size can vary from just a few centimetres, up to the full length of the incision. Most hernias will not require further treatment, but in more severe cases, further surgery may be required to repair the hernia.
Complications within the abdomen
Haemoperitoneum: A rare complication where there is blood within the abdomen from bleeding at the surgical site.
Anastomosis complications: The anastomosis site is where two opposing ends of intestine that have been opened are sutured back together again. It is important that at this site no leakage of intestinal contents occurs. Leakage or breakdown at this site can lead to peritonitis, which is inflammation or infection within the abdominal cavity and is a potentially life threatening complication.
Adhesions: Scar tissue can form within the abdomen following abdominal surgery. Occasionally this may cause further colic episodes
Further colic episodes
Further colic episodes can occur following surgery. These can occur days to months following discharge.
Endotoxaemia
In some rare cases, horses may develop sepsis in response to toxins released by damaged intestine
Diarrhoea
This is a rare complication. It can develop as a result of infections with C. difficile or Salmonella. As a consequence, some horses may need to be treated in isolation to ensure infection doesn’t spread to other horses or humans.
Post-operative ileus
Post-operative ileus is one of the potential post-operative complications which can lead to a significant increase in hospital stay duration, increased treatment costs and is also associated with reduced survival rates. Post-operative ileus is a condition that affects the muscle function in the intestinal wall. The intestine is a long tube-like structure that has a muscular wall throughout its entire length from the oesophagus to the anus. The function of this muscle is to contract in waves to mix and move food along the length of the intestinal tract, within which digestion occurs and nutrients are absorbed, terminating in the excretion of waste material as faeces. In post-operative ileus these contractions stop and thus intestinal contents are not moved throughout the intestinal tract. In most cases, it is transient and lasts for up to 48 hours following surgery; however, in some cases it can last longer. A build-up of fluid develops within the intestine as a result of the lack of propulsion. This stretches the intestines and stomach, resulting in pain and the horse’s inability to eat. Unlike humans, the horse is unable to vomit; consequently, this excess fluid must be removed from the stomach by other means, otherwise there is a risk of the stomach rupturing with fatal consequences. Post-operative ileus may occur in up to 60% of horses undergoing abdominal surgery and mortality rates as high as 86% have been reported. Horses in which the small intestine manipulated is extensively manipulated during surgery and those that require removal of segments of intestine are at higher risk. Despite the significant risk of post-operative ileus following colic surgery in horses, there is a lack of studies investigating the mechanisms underpinning this condition in horses; consequently, the precise cause of this condition in horses is not fully known.
What causes the intestine to stop functioning?
For many years it was thought that post-operative ileus occurred as a result of a dysfunction of the nerves that stimulate contraction of the muscles in the intestinal wall. This theory has now mostly been superseded by the concept that it primarily results from inflammation in the intestinal wall. Based on human and rodent studies, it has been shown that immune cells in the intestine (macrophages) play a key role in development of this condition. Macrophages are important cells found everywhere in the body, with the largest population being in the intestine. These cells become activated by the inevitable manipulation of the horses’ intestines during colic surgery, with subsequent initiation of a sequence of events which ultimately results in dysfunction of the muscle in the intestinal wall. We know macrophages are present within the wall of the horses’ intestine and that at the time of colic surgery there is an inflammatory response at this site. Although the significance of these findings in relation to post-operative ileus in the horse remains unknown, they provide sufficient justification for ongoing research focused on the inflammatory response in the intestine of horses during and immediately following colic surgery…


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Conformation and Breeding Choices

By Judy Wardrope
A lot of factors go into the making of a good racehorse, but everything starts with the right genetic combinations; and when it comes to genetics, little is black and white. The best we can do is to increase our odds of producing or selecting a potential racehorse. Examining the functional aspects of the mare and then selecting a stallion that suits her is another tool in the breeding arsenal.
For this article we will use photos of four broodmares and analyze the mares’ conformational points with regard to performance as well as matings likely to result in good racehorses from each one. We will look at qualities we might want to cement and qualities we might hope to improve for their offspring. In addition, we will look at their produce records to see what has or has not worked in the past.
In order to provide a balance between consistency and randomness, only mares that were grey (the least common color at the sale) with three or more offspring that were likely to have had a chance to race (at least three years old) were selected. In other words, the mares were not hand-picked to prove any particular point.
All race and produce information was taken from the sales catalogue at the time the photos were taken (November 2018) and have not been updated.

Mare 1
Her lumbosacral gap (LS) (just in front of the high point of croup, and the equivalent of the horse’s transmission) is not ideal, but within athletic limits; however, it is an area one would hope to improve through stallion selection. One would want a stallion with proven athleticism and a history of siring good runners.
The rear triangle and stifle placement (just below sheath level if she were male) are those of a miler. A stallion with proven performance at between seven furlongs and a mile and an eighth would be preferable as it would be breeding like to like from a mechanical perspective rather than breeding a basketball star to a gymnast.
Her pillar of support emerges well in front of the withers for some lightness of the forehand but just behind the heel. One would look for a stallion with the bottom of the pillar emerging into the rear quarter of the hoof for improved soundness and longevity on the track. Her base of neck is well above her point of shoulder, adding additional lightness to the forehand, and she has ample room behind her elbow to maximise the range of motion of the forequarters. Although her humerus (elbow to point of shoulder) shows the length one would expect in order to match her rear stride, one would likely select a stallion with more rise from elbow to point of shoulder in order to add more lightness to the forehand.
Her sire was a champion sprinter as well as a successful sire, and her female family was that of stakes producers. She was a stakes-placed winner at six furlongs—a full-sister to a stakes winner at a mile as well as a half-sister to another stakes-winning miler. Her race career lasted from three to five.
She had four foals that met the criteria for selection; all by distance sires of the commercial variety. Two of her foals were unplaced and two were modest winners at the track. I strongly suspect that this mare’s produce record would have proven significantly better had she been bred to stallions that were sound milers or even sprinters.

Mare 2
Her LS placement, while not terrible, could use improvement; so one would seek a stallion that was stronger in this area and tended to pass on that trait.
The hindquarters are those of a sprinter, with the stifle protrusion being parallel to where the bottom of the sheath would be. It is the highest of all the mares used in this comparison, and therefore would suggest a sprinter stallion for mating.
Her forehand shows traits for lightness and soundness: pillar emerging well in front of the withers and into the rear quarter of the hoof, a high point of shoulder plus a high base of neck. She also exhibits freedom of the elbow. These traits one would want to duplicate when making a choice of stallions.
However, her length of humerus would dictate a longer stride of the forehand than that of the hindquarters. This means that the mare would compensate by dwelling in the air on the short (rear) side, which is why she hollows her back and has developed considerable muscle on the underside of her neck. One would hope to find a stallion that was well matched fore and aft in hopes he would even out the stride of the foal.
Her sire was a graded-stakes-placed winner and sire of stakes winners, but not a leading sire. Her dam produced eight winners and three stakes winners of restricted races, including this mare and her full sister.
She raced from three to five and had produced three foals that met the criteria for this article. One (by a classic-distance racehorse and leading sire) was a winner in Japan, one (by a stallion of distance lineage) was unplaced, and one (by a sprinter sire with only two starts) was a non-graded stakes-winner. In essence, her best foal was the one that was the product of a type-to-type mating for distance, despite the mare having been bred to commercial sires in the other two instances.
Mare 3 ….


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Antimicrobial resistance

By Jennifer Davis and Celia Marr

Using antimicrobials as effectively as possible helps to reduce their use overall. For septic arthritis, intravenous regional perfusion of antimicrobials can achieve very high concentrations within a specific limb. This involves placing a temporary tourniquet to reduce blood flow away from the area while the antimicrobial is injected into a nearby blood vessels. The technique is suitable for some but not all antimicrobial drugs.
Growing numbers of bacterial and viral infections are resistant to antimicrobial drugs, but no new classes of antibiotics have come on the market for more than 25 years. Antimicrobial-resistant bacteria cause at least 700,000 human deaths per year according to the World Health Organization (WHO). Equivalent figures for horses are not available, but where once equine vets would have very rarely encountered antimicrobial-resistant bacteria, in recent years this serious problem is a weekly, if not daily, challenge.
The WHO has for several years now, designated a World Antibiotic Awareness Week each November and joining this effort, British Equine Veterinary Association and its Equine Veterinary Journal put together a group of articles exploring this problem in horses.
How do bacterial populations develop resistance?
Certain types of bacteria are naturally resistant to specific antimicrobials and susceptible to others. Bacteria can develop resistance to antimicrobials in three ways: bacteria, viruses and other microbes, which can develop resistance through genetic mutations or by one species acquiring resistance from another. Widespread antibiotic use has made more bacteria resistant through evolutionary pressure—the “survival of the fittest” principle means that every time antimicrobials are used, susceptible microbes may be killed; but there is a chance that a resistant strain survives the exposure and continues to live and expand. The more antimicrobials are used, the more pressure there is for resistance to develop.
The veterinary field remains a relatively minor contributor to the development of antimicrobial resistance. However, the risk of antimicrobial-resistant determinants travelling between bacteria, animals and humans through the food chain, direct contact and environmental contamination has made the issue of judicious antimicrobial use in the veterinary field important for safeguarding human health. Putting that aside, it is also critical for equine vets, owners and trainers to recognise we need to take action now to limit the increase of antimicrobials directly relevant to horse health.
How does antimicrobial resistance impact horse health?

This mare’s problems began with colic; she underwent surgery to correct a colon torsion (twisted gut). When the gut wall is damaged, bacteria easily spread throughout the body. The mare developed an infection in her surgical incision and in her jugular veins, progressing eventually to uncontrollable infection—resistant to all available antimicrobials with infection of the heart and lungs.
The most significant threat to both human and equine populations is multidrug-resistant (MDR) pathogens, including methicillin-resistant Staphylococcus aureus (MRSA), extended-spectrum beta-lactamase (ESBL) producing Escherichia coli, MDR Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, and rising MDR strains of Salmonella spp. and Clostridium difficile. In an analysis of 12,695 antibiograms collected from horses in France between 2012-2016, the highest proportion (22.5%) of MDR isolates were S. aureus. Identification of ESBL E.coli strains that are resistant to all available antimicrobial classes has increased markedly in horses. In a sampling of healthy adult horses at 41 premises in France in 2015, 44% of the horses shed MDR E.coli, and 29% of premises shedding ESBL isolates were found in one third of the equestrian premises. Resistant E. coli strains are also being found in post-surgical patients with increasing frequency.

Rhodococcus equi is a major cause of illness in young foals. It leads to pneumonia and lung abscesses, which in this example have spread through the entire lung. Research from Kentucky shows that antimicrobial resistance is increasingly common in this bacterial species.
Of major concern to stud owners, antimicrobial-resistant strains of Rhodococcus equi have been identified in Kentucky in the last decade, and this bacteria can cause devastating pneumonia in foals. Foals that are affected by the resistant strains are unlikely to survive the illness. One of the leading authorities on R equi pneumonia, Dr Monica Venner has published several studies showing that foals can recover from small pulmonary abscesses just as quickly without antibiotics, and has pioneered an ‘identify and monitor’ approach rather than ‘identify and treat’. Venner encourages vets to use ultrasonography to quantify the infected areas within the lung and to use repeat scans, careful clinical monitoring and laboratory tests to monitor recovery. Antimicrobials are still used in foals, which are more severely affected, but this targeted approach helps minimise drug use.
What can we do to reduce the risk of antimicrobial resistance?

Faced with a coughing horse, trainers will often pressure their vet to administer antibiotics, hoping this will clear the problem up quickly. Many respiratory cases will recover without antibiotics, given rest and good ventilation.
The simple answer is stop using antimicrobials in most circumstances except where this is absolutely avoidable. In training yards, antimicrobials are being over-used for coughing horses. Many cases are due to viral infection, for which antibiotics will have little effect. There is also a tendency for trainers to reach for antibiotics rather than focusing on improving air quality and reducing exposure to dust. Many coughing horses will recover without antibiotics, given time. Although it has not yet been evaluated scientifically, adopting the ‘identify and monitor’ approach, which is very successful in younger foals, might well translate to horses in training in order to reduce overuse of antimicrobials.
Vets are also encouraged to choose antibiotics more carefully, using laboratory results to select the drug which will target specific bacteria most effectively. The World Health Organization has identified five classes of antimicrobials as being critically important, and therefore reserved, antimicrobials in human medicine. The critically important antimicrobials which are used in horses are the cephalosporins (e.g., ceftiofur) and quinolones (e.g., enrofloxacin), and the macrolides, which are mainly used in foals for Rhodococcal pneumonia. WHO and other policymakers and opinion leaders have been urging vets and animal owners to reduce their use of critically important antimicrobials for well over a decade now. Critically important antimicrobials should only be used where there is no alternative, where the disease being treated has serious consequences and where there is laboratory evidence to back up the selection. British Equine Veterinary Association has produced helpful guidelines and a toolkit, PROTECT-ME, to help equine vets achieve this.
How well are we addressing this problem?….


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Roarers - surgery for recurrent laryngeal neuropathy – impact and outcomes

By Safia Barakzai BVSc MSc DESTS Dipl.ECVS
Recurrent laryngeal neuropathy (RLN), more commonly known as ‘roaring’, ‘laryngeal paralysis’ and ‘laryngeal hemiplegia’ is a disorder affecting primarily the left recurrent laryngeal nerve in horses >15hh. This nerve supplies the muscles that open and close the left side of the larynx. The right recurrent laryngeal nerve is also now proven to be affected, but only very mildly, thus affected horses very rarely show signs of right-sided dysfunction.
Horses with RLN become unable to fully open (abduct) the left side of their larynx. During exercise they then make abnormal inspiratory noise due to collapse of both the vocal fold(s) and the left arytenoid cartilage (figure 1), and airflow to the lungs can become severely obstructed in advanced cases. There is a proven genetic component to RLN, but in many cases the disease progresses over months or years. The age at which clinical signs become apparent is highly variable. Foals can show endoscopic and pathologic evidence of RLN, but some horses do not develop clinical disease until >10 years old.
Treatment of RLN

Laryngoplasty (tie-back) being performed in standing sedated horses.
Traditionally, left-sided ventriculocordectomy (‘Hobday’/ventriculectomy plus vocal-cordectomy surgery) and laryngoplasty (‘tie-back’) surgeries have been used to treat the disorder, depending on which structures are collapsing and how severely. The intended use of the horse, the budget available and other concerns of the owner/trainer also come into play. New techniques of providing a new nerve supply (‘re-innervating’) to the affected muscle are now being trialled in clinical cases. Pacing the muscle with an implanted electronic device has also been attempted in research cases.
Ventriculocordectomy
Ventriculocordectomy is commonly now referred to as a ‘Hobday’ operation; however, the ‘Hobday’ actually only refers to removal of the blind ending sac that constitutes the laryngeal ventricle. Currently, surgeons tend to remove the vocal cord as well as the ventricle, because it is vocal cord collapse that creates the ‘whistling’ noise. It is a relatively straightforward surgery to perform with minimal risks and complications for the patient. In the last 15 years, there has been a shift to performing it in a minimally invasive way, using a diode laser under endoscopic guidance in the standing sedated horse rather than with the conventional method, via an open laryngotomy incision on the underside of the neck with the horse under a general anaesthetic. However, transendoscopic laser surgery is technically difficult with a very steep learning curve for the surgeon. All ventriculocordectomies are not equal (Fig. 2) and for both laser and ‘open surgery’ methods, incomplete resection of the fold can leave behind enough tissue to cause ongoing respiratory noise and/or airway obstruction after surgery.
Severity of disease can be reasonably estimated using endoscopy in the resting horse (grades 1-4), but the gold standard for assessing this disease is endoscopy during exercise, when the high negative pressure—generated when breathing—test the affected laryngeal muscle, which is trying its best to resist the ‘suction’ effect of inspiration.
During exercise, RLN is graded from A to D, depending on how much the left side of the larynx can open.

Figure 2: Two horses after ventriculocordectomy surgery. The horse on the left has an excellent left-sided ventriculocordectomy, with complete excision of the vocal fold tissue (black arrow). The right cord is intact, but the right ventricle has been removed (‘Hobday’). The horse on the right has bilaterally incomplete vocalcordectomies, with much of the vocal fold tissue left behind.
Sports horses, hunters and other non-racehorses were often previously recommended to have a ventriculocordectomy performed rather than a laryngoplasty, even if they had severe RLN. This decision was often made on the grounds of cost, but also due to fear of complications associated with laryngoplasty (‘tie-back’ surgery). A new study has shown that for horses with severe RLN, a unilateral ventriculocordectomy is actually extremely unlikely to eliminate abnormal noise in severely affected horses, because the left arytenoid cartilage continues to collapse.3 The authors recommended that laryngoplasty plus ventriculocordectomy is a better option than ventriculocordectomy alone for all grade C and D horses if resolution of abnormal respiratory noise and significant improvement of the cross sectional area of the larynx are the aims of surgery.
Advancements in laryngoplasty (‘tie-back’) surgery
Laryngoplasty is indeed one of the most difficult procedures that equine surgeons perform ….


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
What is equine welfare? Asks Johnston Racing’s vet Neil Mechie

Neil Meche
The world of equine welfare—and animal welfare in general—is a proverbial can of worms. Decisions regarding equine welfare must be made on logical scientific evidence and not be biased by emotion or fear of incorrect perceptions in the media or public eye. As with many things in life, education is the key, especially in a world where large parts of the population have very little experience or knowledge of keeping or working with animals.
The welfare of animals is protected in national legislation in the UK. The Animal Welfare Act 2006 makes owners and keepers responsible for ensuring that the welfare needs of their animals are met. These include the need:
for a suitable environment (place to live)
for a suitable diet (food and water)
to exhibit normal behaviour patterns
to be housed with, or apart from, other animals (if applicable)
to be protected from pain, injury, suffering and disease
Reading these concise bullet points, one would think it quite simple to meet these needs, but issues arise when it comes to interpreting and putting this guidance into practice.
As an insight into how emotive language can change the interpretation of animal welfare requirements, below are the The Royal Society for the Prevention of Cruelty to Animals (RSPCA) “Five Freedoms,” which are not too dissimilar to the above but portrayed in a different light:
Freedom from hunger and thirst
Freedom from discomfort
Freedom from pain, injury or disease
Freedom to express normal behaviour
Freedom from fear and distress

The RSPCA is a charity champions animal welfare, and the use of words such as hunger, thirst, discomfort, fear and distress conjure up images of tortured animals wasting away in squalor. There is no need for this dramatic language when the preservation of welfare only actually requires common sense and compassion.
The same can be said when considering the welfare of horses, but sadly this is not the case. The biggest welfare issues facing the horse population are not, as the media would have you think, horses breaking their legs on racetracks or the travelling community mistreating horses at Appleby Fair. It is obesity and the mis-management of horses in the general population. Every day horses are being killed by a plethora of issues caused by over-feeding and poor management regimes. Laminitis, colic and numerous hormonal and metabolic diseases negatively affect the welfare of thousands of horses each year and are in a large part caused by the poor knowledge and horsemanship of their owners. It is now a large part of most equine vets’ job to educate horse owners on appropriate feeds and management regimes for their horses.
Racehorses, on the contrary, are looked after with the highest of standards as they are athletes competing at a high level.


BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Planning a diagnostic-led worm control programme

Common horse worms
By Dr Corrine Austin (Austin Davis Biologics) and Prof Jacqui Matthews (Roslin Technologies)
Planning a diagnostic-led worm control programme
All horses are exposed to worms while grazing, but how we control these parasites is essential to horse health and performance. Most horse owners are aware of testing to determine whether their horse needs deworming. The tests comprise faecal worm egg counts (FEC) for redworm/roundworm detection and saliva testing to detect tapeworm infections (standard FEC methods are unreliable for tapeworm). Until now, encysted small redworm larvae have remained undetectable as FEC only determines the presence of egg laying adult worms. This has meant that routine winter moxidectin treatment has become recommended practice to target potentially life-threatening burdens of small redworm encysted larvae. Excitingly, a new small redworm blood test is being commercialised* which detects all stages of the small redworm life cycle, including the all-important encysted larval phase. Together, these tests offer a complete worm control programme for common horse worms using diagnostic information. This is known as ‘diagnostic-led worm control’ (see Figure 1 for common worms in horses). Essentially, testing is used to tell you whether your horse needs deworming or not.
Why should you use testing to determine whether you should use dewormers or not?
Gone are the days of routinely administering dewormers to every horse and hoping for the best. That strategy is outdated as it has caused widespread drug resistance in worms (i.e., worms are able to survive the killing effects of dewormers and remain in place after treatment, which can lead to disease and in worst cases, death). To reduce the risk of further resistance occurring, we need to ensure that dewormers are only used when they are genuinely needed—when testing detects that horses have a worm burden requiring treatment. Regular testing also helps identify horses likely to be more susceptible to infection and thus at risk of disease in the future.
How to plan your horse’s worm control programme ….
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Bleeders - the facts, fiction and future direction
By Dr. David Marlin

We are now approaching half a century since Bob Cook pioneered the use of the flexible fibreoptic endoscope, which allowed examination of the respiratory tract in the conscious horse. One of the important outcomes of this technique was that it opened the door to the study of ‘bleeding’ or exercise-induced pulmonary haemorrhage (EIPH). But nearly 50 years on the irony is perhaps that whilst we have become good at describing the prevalence of EIPH and some of the factors that appear to increase the severity of EIPH within individual horses, we still lack a clear understanding of the condition and how to manage it. I use the term manage rather than treat or prevent as our knowledge of EIPH must show us that EIPH cannot be stopped entirely; it is a consequence of intense exercise. The other irony is that in the past 50 years, by far the majority of research into the management of EIPH has focussed on the use of the diuretic furosemide. Whilst we have good evidence from controlled studies that furosemide reduces the severity of EIPH on a single occasion, we still lack good evidence to suggest that furosemide is effective when used repeatedly during training and or racing; and there is also evidence to the contrary.
Let’s review some basic facts about EIPH, which should not be contentious.
EIPH is the appearance of blood in the airways associated with exercise.
EIPH occurs as a result of moderate to intense exercise. In fact, EIPH has been found after trotting when deep lung wash (bronchoalveolar lavage or BAL) is done after exercise.
EIPH most often involves the smallest blood vessels (capillaries) but can sometimes and less commonly be due to the rupture of larger blood vessels.
The smallest blood vessels are extremely thin. Around 1/100th the thickness of a human hair. But this extremely thin membrane is also what allows racehorses such as thoroughbreds, standardbreds and Arabs to use oxygen at such a high rate and is a major reason for their athleticism.
EIPH is a progressive condition. The chance of seeing blood in the trachea after exercise increases with time in racing.
EIPH is variable over time, even when horses are scoped after the same type of work.
If you ‘scope a horse after three gallops in a row, you can expect to see blood in the trachea on at least one occasion.
EIPH damage to the lungs starts at the back and top, and over time moves forward and down and is approximately symmetrical.
Following EIPH the lung becomes fibrotic (as scar tissue), stiffer and does not work as well. The iron from the blood is combined with protein and stored permanently in the lung tissue where it can cause inflammation.
High blood pressure within the lung is a contributing factor in EIPH. Horses with higher blood pressure appear to suffer worse EIPH.
There is also evidence that upper airway resistance and breathing pattern can play a role in EIPH.
Airway inflammation and poor air quality may increase the severity of EIPH within individual horses.
Increasing severity of EIPH appears to have an increasing negative effect on performance.
Visible bleeding (epistaxis) has a very clear and marked negative effect on performance.
In order to make progress in the management of EIPH (i.e., to minimise the severity of EIPH in each individual), there are certain steps that trainers can take based on the information we have to date.
These include:

Ensuring good air quality in stables
Regular respiratory examination and treatment of airway inflammation
Reduced intensity of training during periods of treatment for moderate to severe airway inflammation
Extended periods of rest and light work with a slower return to work for horses following viral infection
Addressing anything that increases upper airway resistance (e.g., roaring, gurgling)
Avoiding intense work in cold weather
Avoiding extremes of going
Limiting number of training days in race preparation and increasing interval between races

Endoscopy
FUTURE OPPORTUNITIES IN UNDERSTANDING AND MANAGING EIPH
We have to accept EIPH as a normal consequence of intense exercise in horses. Our aim should be to reduce the severity to a minimum in each individual horse. However, there are areas in which we still need a much greater scientific understanding.
What actually causes the capillaries to leak or rupture?…
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
An Introduction to the Functional Aspects of Conformation

By Judy Wardrope
Why is one horse a sprinter and another a stayer? Why is one sibling a star and another a disappointment? Why does one horse stay sound and another does not? Over the course of the next few issues, we will delve into the mechanics of the racehorse to discern the answer to these questions and others. We will be learning by example, and we will be using objective terminology as well as repeatable measures. This knowledge can be applied to the selection of racing prospects, to the consideration of distance or surface preferences and, of course, to mating choices.
Introducing a different way of looking at things requires some forethought. Questions need to be addressed in order to provide educational value for the audience. How does one organise the information, and how does one back up the information? In the case of equine functionality in racing, which horses will provide the best corroborative visuals?



After considerable thought, these three horses were selected: Tiznow (Horse #1) twice won the Breeders’ Cup Classic (1¼ miles) ; Lady Eli (Horse #2) won the Juvenile Fillies Turf and was twice second in the Filly and Mare Turf (13/8 miles); while our third example (Horse #3) did not earn enough to pay his way on the track. Let’s see if we can explain the commonalities and the differences so that we can apply that knowledge in the future.
Factors for Athleticism
If we consider the horse’s hindquarters to be the motor, then we should consider the connection between hindquarters and body to be the horse’s transmission. Like in a vehicle, if the motor is strong, but the transmission is weak, the horse will either have to protect the transmission or damage it.
According to Dr. Hilary M. Clayton (BVMS, PhD, MRCVS), the hind limb rotates around the hip joint in the walk and trot and around the lumbosacral joint in the canter and gallop. “The lumbosacral joint is the only part of the vertebral column between the base of the neck and the tail that allows a significant amount of flexion [rounding] and extension [hollowing] of the back. At all the other vertebral joints, the amount of motion is much smaller. Moving the point of rotation from the hip joint to the lumbosacral joint increases the effective length of the hind limbs and, therefore, increases stride length.” From a functional perspective, that explains why a canter or gallop is loftier in the forehand than the walk or the trot.
In order to establish an objective measure, I use the lumbosacral (LS) gap, which is located just in front of the high point of the croup. This is where the articulation of the spine changes just in front of the sacrum, and it is where the majority of the up and down motion along the spine occurs. The closer a line drawn from the top point of one hip to the top point of the other hip comes to bisecting this palpable gap, the stronger the horse’s transmission. In other words, the stronger the horse’s coupling.

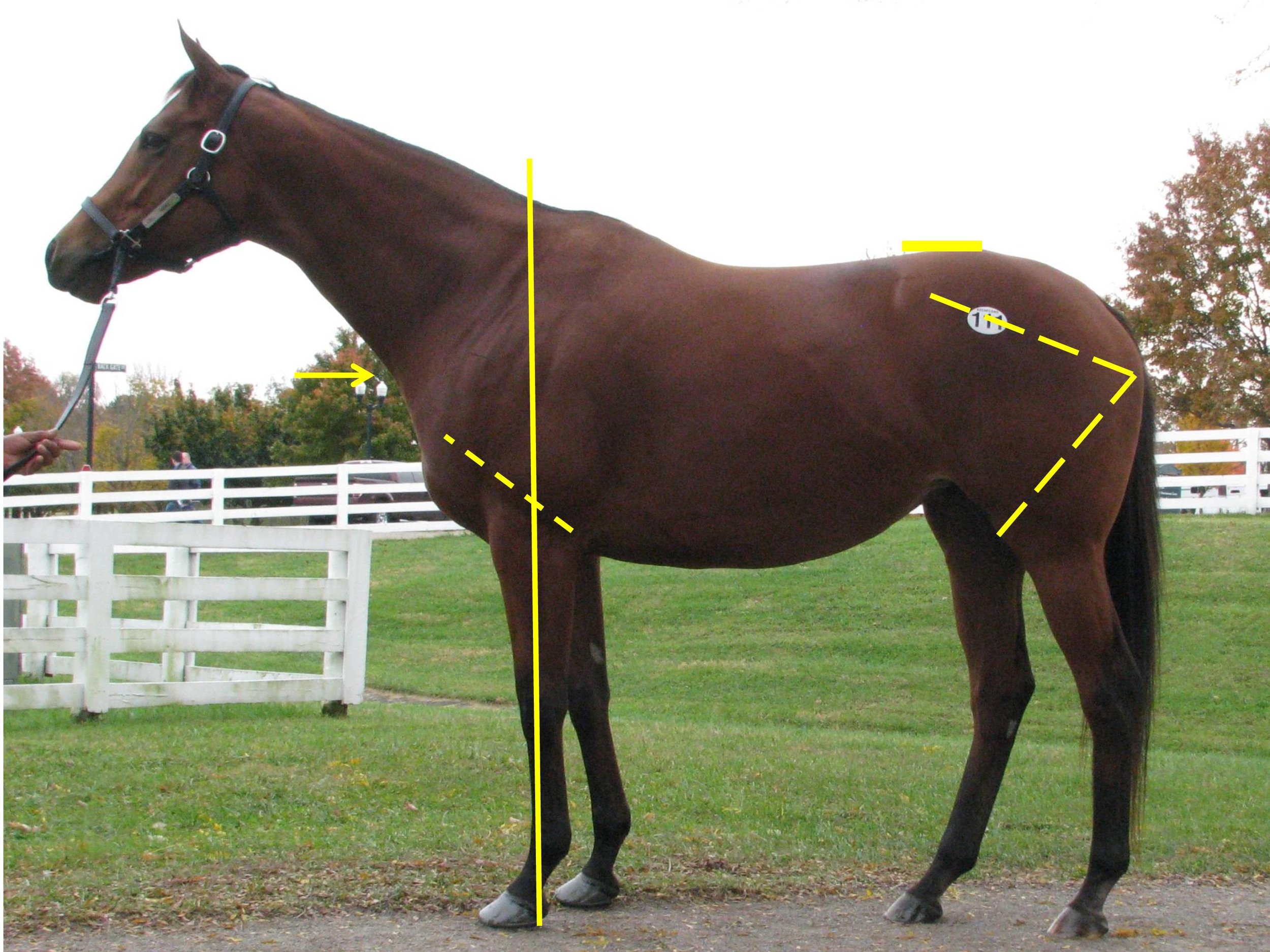
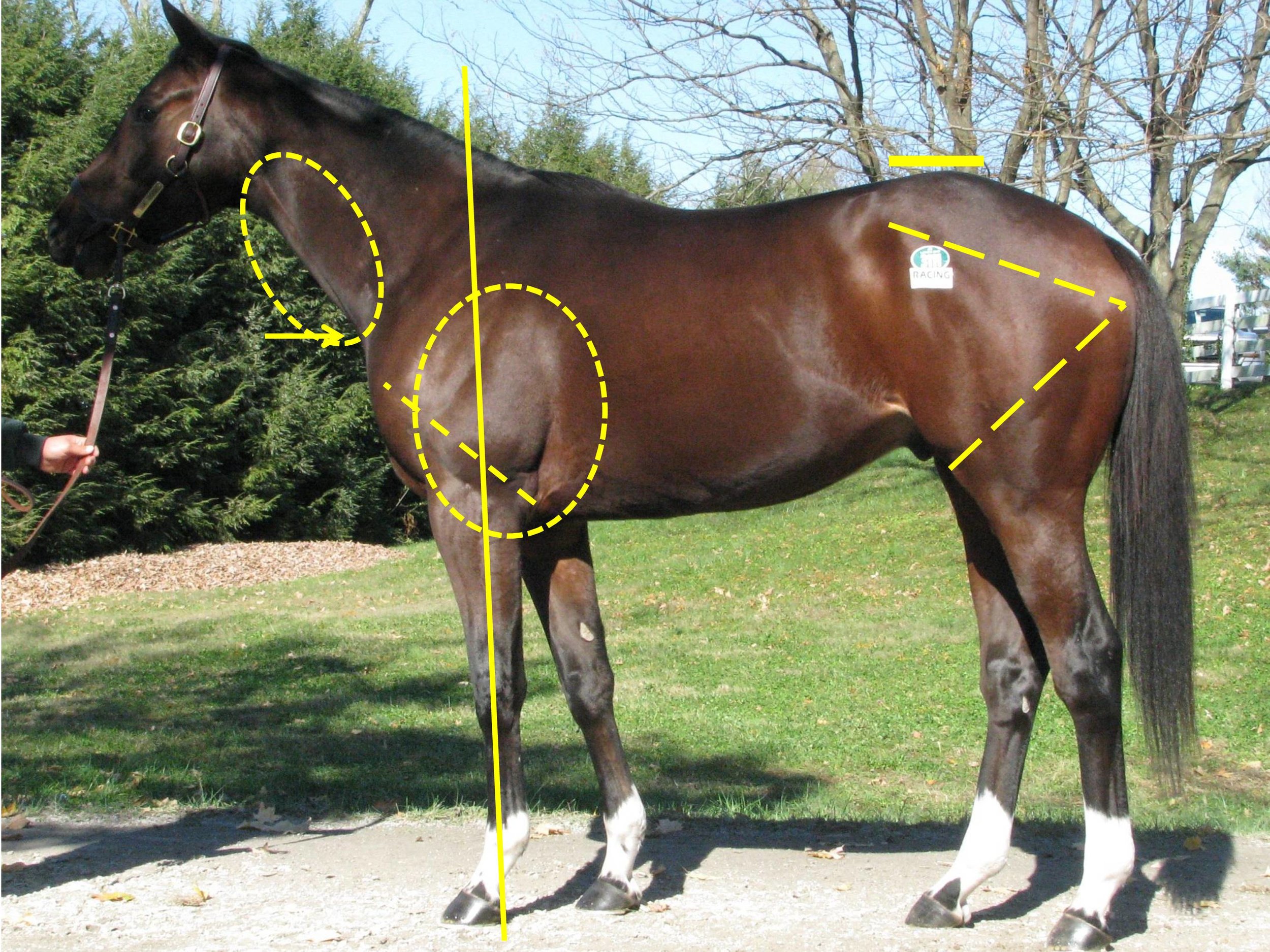
We can see that the first two horses have an LS gap (just in front of the high point of the croup as indicated) that is essentially in line with a line drawn from the top of one hip to the top of the opposing hip. This gives them the ability to transfer their power both upward (lifting of the forehand) and forward (allowing for full extension of the forehand and the hindquarters). Horse #3 shows an LS gap considerably rearward of the top of his hip, making him less able to transfer his power and setting him up for a sore back.
You may also notice that all three of these sample horses display an ilium side (point of hip to point of buttock), which is the same length as the femur side (point of buttock to stifle protrusion)—meaning that they produce similar types of power from the rear spring as it coils and releases when in stride. We can examine the variances in these measures in more detail in future articles, when we start to delve into various ranges of motion as well as other factors for soundness or injury.
Factors for Distance Preferences…
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Equine Pain: how can we recognise it and which painkiller should we use?

By Professor Celia Marr
We can all agree that alleviating pain in our patients is an important goal, but we may not be as good as we might hope at recognising pain in horses. Studies have shown that there is considerable variation in the scores vets assign when asked to predict how much pain they expect to see with specific clinical conditions.
Acute severe pain is perhaps most easily recognised by horsemen and vets; signs of severe colic, such as rolling, are usually very obvious. Low-grade pain, and pain not associated with abdominal disease can be more difficult to detect and go unrecognised. In particular, intra-thoracic pain and pain associated with injuries to the thoracic cage, withers and spine can be difficult to pinpoint.

This horse is clearly showing signs of abdominal pain—colic. It is lying down, has been rolling and is looking at its flank.
Comfortable horses interact with their environment, look out over their stable door and eat willingly. Reluctance to move and restlessness indicate pain while looking at the flank, and kicking at the abdomen all suggest localised pain. Behaviours such as lifting hindlimbs, extending head, lateral and/or vertical head movements and pawing are also observed in uncomfortable horses.
Facial expression and pain
In humans, facial expressions are an important part of nonverbal communication. The Horse Grimace Scale has been developed to help identify subtle pain in horses. The grimace scale is easy to learn, can be applied quickly and takes into account our natural human tendency to focus on the face when evaluating both human and non-humans around us. This scale looks at ear position, tension around the eyes, tension in the chewing muscles and shape of the nostrils which tend to be held in a strained position if in pain. More complex pain scales incorporate facial expression with head position, flehmen, yawning, teeth grinding and interaction with people.


These scales were used in a recent Equine Veterinary Journal article looking at optimal methods to provide anaesthesia for castration. But, the focus on a strained facial expression, ears held back and lack of interaction with people can easily be misinterpreted as poor temperament. It is well worth trainers taking time to make sure their staff are educated on how to recognise signs of pain, as these sorts of clinical signs might indicate important conditions such as gastric ulcers, pneumonia or even musculoskeletal conditions such as fractured ribs. Yard staff should be encouraged to give horses the benefit of the doubt and report any apparent poor temperament so that veterinary investigations can be undertaken to get to the bottom of the problem. Similarly, these signs can be used to monitor horses after potentially painful procedures such as following surgery or castration.
What do we know about analgesic use in equine practice?
There is an increasingly large number of painkillers, also known as analgesics, which are either licensed for use in the horse or supported by research evidence. But it is likely that most equine vets use a relatively small range. British Equine Veterinary Association (BEVA) has recently tasked a team of its members to look at the evidence with underpin best practice for selections of analgesics in common clinical scenarios. This group is chaired by Professor Mark Bowen of the University of Nottingham and has been working for two years now and has collected evidence from the veterinary literature; and in parallel the group has consulted BEVA members to develop robust recommendations. The BEVA Clinical Practice Guidelines report on analgesia will be published soon and looks at the most effective analgesia in horses undergoing routine castration, horses with acute colic, orthopaedic pain and in horses with chronic pain that does not respond to standard non-steroidal anti-inflammatory drugs (NSAIDs) such as phenylbutazone (aka “Bute”). In making their recommendations around use of analgesics in horses, the BEVA team considered both the effectiveness of each analgesic drug, its safety and potential for side-effects.
What are the desirable characteristics of analgesic drugs?
The ideal analgesic has predictable effect and duration, minimal side effects and is easy to prescribe, purchase and administer, lacking any impact on the horse’s future status for human consumption. Of course, the ideal analgesic does not exist. To a large extent, the most appropriate analgesic will be dictated by the specific clinical indication.
Analgesia in colic
With colic, predictable level of analgesia and duration of action are key characteristics. The BEVA team found moderate evidence that flunixin provides superior analgesia to meloxicam and phenylbutazone in horses with colic. However, effective analgesia is desirable but very potent drugs are usually avoided for fear of masking declining clinical status in a horse which would be best served by surgical exploration rather than controlled with extremely potent analgesics. Potential damage to the gastrointestinal tract and effects on gastrointestinal motility are critical and the impact of concurrent shock and volume depletion must be considered. Similar considerations come into play with peri-operative pain but here, the level of analgesia required may be modified by the exact surgical indication and specific procedure and with some procedures, it will be appropriate to provide very potent analgesia, for example with surgical repair of fractures or other painful orthopaedic surgeries. In these cases, multimodal analgesia may well be indicated.
Analgesia following castration
The BEVA team found robust evidence to support a recommendation that pre-operative NSAIDs should be administered prior to surgery. They also recommended that analgesia should be given for at least three days after surgery and that local anaesthetic should be infused into the testicle even when a general anaesthetic is administered. Finally, they counselled that pre-operative use of butorphanol (a commonly used component of sedative protocols) alone should not be considered adequate analgesia for horses undergoing castration.
Selection of NSAIDs for musculoskeletal pain
There is moderate evidence to indicate that phenylbutazone provides superior analgesia for hoof pain / laminitis, compared to firocoxib and meloxicam but strong evidence to show that Suxibuzone can be used as a direct replacement for phenylbutazone in chronic orthopaedic pain. The evidence supporting the use of other NSAIDs is less definitive. Meloxicam and firocoxib may be equivalent to phenylbutazone for pain associated with inflammation of the joint lining and, although studies are not conclusive, the group came to the conclusion that ketoprofen is not as effective for addressing musculoskeletal pain.
One of the key safety recommendations relating to the use of phenylbutazone was that it is the NSAID that is most likely to induce gastrointestinal adverse events (right dorsal colitis or gastric glandular ulceration). However, although other NSAIDs have less adverse intestinal effects but can all be considered as potentially ulcerogenic. Horses on long-term analgesic therapy should be monitored carefully and further investigations undertaken if they show weight loss, poor appetite or develop the more general signs of pain described above, as this might indicate that the NSAID is having adverse effects on the intestine.
The BEVA team also concluded that giving NSAIDs at doses above those generally recommended in veterinary texts and stacking (i.e., combining maximal doses of different NSAIDs) should be avoided. These practices simply increase risk with no analgesic benefit.
Alternative analgesics
Unfortunately, there are not many practical alternatives to NSAIDs. There is research ongoing looking at topical NSAIDs and alternative drugs such as paracetamol, tramadol and fentanyl. These drugs are unlikely to be in common use in horses in training but do have a place in management of horses with more severe clinical problems.
Similarly, morphine and methadone are used commonly in equine hospitals, but these Schedule 2 controlled drugs are generally not used widely in practice. Buprenorphine has been extensively researched recently and evidence is accumulating supporting its use particularly in the peri-operative patient.
Final warnings
The BEVA group’s report contained a clear warning that highly potent analgesia should only be utilised under the direct control of a veterinary surgeon who has fully evaluated a horse and having developed a therapeutic, analgesic plan that includes ongoing monitoring. It is also important to bear in mind that the best way to alleviate pain associated with a specific clinical condition is to cure the underlying cause. Painkillers should always be used with respect and not be seen as a way to patch up a horse that has an undiagnosed musculoskeletal problem or internal condition.
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!

Post-Race Collapse - Prevention & Management
By Dr. David Marlin
Fortunately, incidents of post-race collapse are relatively rare following racing, however if they do occur, it’s important to know what steps can be taken. Common causes of post-race collapse include cardiac arrhythmias, neurologic events, internal bleeding due to large blood vessel rupture, airway obstruction and overheating. All of these are a serious cause for concern and likely to require veterinary support. However, overheating is likely to be one of the most common reasons for post-race collapse, but it is often not recognised as such and can lead to horses not receiving prompt treatment that may ensure a swift and uneventful recovery with no long-lasting injury.
During races, horses get hot because for every unit of energy they use which makes the muscles contract, four times as much energy is produced as heat. The harder and longer the horse works, the more heat it produces. Although horses lose heat by sweating (around 85%) and through breathing (around 15%) during a race, around 90% or more of the heat produced is stored in the muscles. Even so, on a hot day, horses may come in at the end of a race with body temperatures 1-2°C higher than they would for the same race in cool conditions.
It would not be unusual for horses to finish races with rectal temperatures of 40-41°C. But taking rectal temperature can also mislead us as the temperature inside the working muscles may be much higher; and it can take five minutes for the rectal temperature to reach a peak after a horse pulls up, increasing by another 1-2°C. It’s as we get to rectal temperatures of 42°C that the risk of collapse due to hyperthermia (high body temperature) becomes significant. Let’s look at why high body temperature can lead to collapse.
Firstly, very high body temperature leads to direct and damaging effects on the brain, the nervous system as a whole and the heart, which may lead to collapse. These effects are related to how high the temperature is and how long the horse stays at that elevated body temperature. For example, if a horse was not cooled off following a race, then it may take 5-10 minutes for the onset of collapse. However, post-race collapse on pulling-up and/or returning to the winners enclosure or stables is not uncommon, and this has a different underlying cause.
During the race, the horse actually reduces blood flow to the skin and chooses instead to send as much as possible to the muscles. This is very different to the situation in people where a significant amount of blood is always sent to the skin to help cooling (thermoregulation). The consequence of blood being directed to the muscles is that the muscle temperatures increase rapidly even over a few minutes of a race. When the horse starts to pull-up, this is reversed and blood is suddenly redirected to the skin. This is most pronounced when the horse comes to a stop. The effect is similar to fainting in people; the flow of blood to the surface causes a fall in blood pressure and effectively the horse faints.
Clearly, collapse of horses is undesirable and has the potential to cause further injury, so it is important to recognise the risks for post-race collapse with respect to overheating and what to do if the situation arises. One of the common misconceptions of post-race collapse is that this is due to “lack of oxygen”. Whilst this could be true in some cases, this is likely to occur in a very small number of horses and only in those with airway obstruction. From studies on treadmills, for example, we know that within a few seconds of starting to slow down, the low oxygen levels in the blood are immediately reversed and even become higher than they were before exercise. People will often cite the ‘blowing’ of horses after a race as an attempt by the horse ‘to get more oxygen in’, however, it’s clear from a number of studies that blowing/breathing after exercise is directly related to body temperature and not oxygen levels. Rapidly reducing body temperature by aggressive cooling results in a more rapid cessation of blowing.
When should heat stress and overheating be suspected? A horse that is hot to touch, blowing very hard and also ataxic (wobbly) when pulled up should be suspected as suffering from overheating, and cooling should be started immediately. If possible avoid turning in tight circles but keep walking as this helps increase blood pressure. Even in cases where overheating is not the main problem, cooling is extremely unlikely to have any negative effects. As mentioned previously, overheating is frequently not considered as a possible cause for post-race ataxia/collapse and may therefore not be recorded as such.
Some time ago Professor Tim Parkin and I examined data from the British Horseracing Authority over three seasons of diagnosed cases of post-race heat stress. Over a three-year period, 108 cases had been recorded by on-course veterinary surgeons post-race. A number of factors significantly increased the risk of a horse suffering overheating. Perhaps not surprisingly, races run in the spring or summer were eight times more likely to include at least one horse with heat stress as races run in the autumn or winter. National Hunt races were almost three times more likely to have a horse with heat stress due to the longer duration of the races compared with the flat. Also, for any type of race, there was an increasing risk for every five furlongs (1,000m). Races run in the afternoon were also three times more likely to have a heat stress case than a race run in the evening. Finally, faster races also increased the risk of horses suffering overheating.
This should all be expected: long races and/or faster races in the afternoon on warm days in spring and summer carry an increased risk of overheating/heat stress and collapse. As not racing in such conditions is not likely to be an option, it’s essential that racecourses and trainers are aware of the signs and risks of overheating and the risk of post-race collapse and take appropriate and prompt action if necessary.
Aggressive cooling is now used extensively in professional endurance racing and eventing, as well as in all equestrian disciplines at major events such as FEI World Championships and Olympic Games. The principle is simple. Applying cold water (0-5°C), either from a hose or from a large container of ice in water, rapidly cools the blood in the skin which in turn more slowly cools the muscles. In horses that are very hot and at risk of heat stroke/collapse, there is no requirement or benefit to scraping water. The key to minimising risk is continuous application of water over as much of the body surface as possible until the breathing starts to recover (i.e., until the blowing reduces). This is the best and most practical indicator of the effectiveness of the cooling. It’s also essential to continue aggressive cooling for 5-10 minutes to bring a horse’s temperature down 1-2°C. As mentioned previously, the cessation of blowing is the best indicator of effective cooling.
Applying cold towels, fans, shade, ice packs on large blood vessels, ice in the rectum, spraying with alcohol are all minimally effective in comparison with continuous application of large volumes of cold water all over the body. In contrast to widely held misconceptions, this approach to cooling does not cause the horse to heat up due to constriction of blood vessels in the skin nor does it cause muscle or kidney damage. The key to preventing collapse and or permanent injury due to heat stroke is rapid instigation of cooling. Literally, seconds count. Delaying cooling by thirty seconds may result in a collapsed horse.
Even in cases where the cause of ataxia/collapse is not primarily due to overheating, starting cooling until veterinary help arrives will not make the situation worse.
Compared with their jockeys, horses are actually able to tolerate much higher body temperatures. A jockey with a temperature of 41°C would be comatose and at risk of serious injury or even death, whilst a horse at 41°C would still be running. However, it is possible for both jockeys and horses to acclimatise to heat. Acclimatisation is the process whereby the body becomes more tolerant of heat as a result of regular daily exercise in the heat. Of course racehorses are most commonly trained early in the morning in the cooler part of the day, yet the majority of races are held in the warmer times of the day, so it’s conceivable that most racehorses are not heat acclimatised. It may also be of interest that heat acclimatisation also improves performance.
In summary, overheating of horses during races is more likely in longer, faster races at warmer times of the year. Horses that are hotter than normal are at an increased risk of heat-related collapse, often when returning to the paddock and standing. Horses that are very hot to touch, blowing hard, wobbly and possibly ‘excited’ are likely to be at risk for collapse. Starting cooling aggressively immediately can lead to rapid recovery and prevent collapse and the risk of more serious injury.
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Advances in Imaging of the Equine Athletic Heart

By Francesca Worsman BVM&S MRCVS
Horserace Betting and Levy Board Senior Clinical Training Scholar in Equine Internal Medicine, Royal (Dick) School of Veterinary Studies, University of Edinburgh
Horses, through selective breeding for athletic excellence, have well-developed hearts that rarely cause problems compared to those encountered by humans. On occasions however, things go wrong. Due to their well-developed physiology, horses are at risk of a fibrillating heart (atrial fibrillation), while circumstantial evidence suggests that more severe heart rhythm abnormalities, somewhat akin to those experienced by human athletes, may cause sudden death. Ultrasound examination of the heart, known as echocardiography is a readily available tool for examining the heart and significant advances in ultrasound technology are likely to provide exciting information about the detailed function of the equine heart. A huge benefit of ultrasound is that it is non-invasive and can be carried out on a standing unsedated horse, so normal heart function is maintained during the examination.
The equine heart, like all mammalian hearts, has four chambers. The right atrium, which receives oxygen-depleted blood from the organs, passes it into the right ventricle which then pumps it to the lungs. Blood picks up oxygen in the lungs and then returns it to the left atrium, which then passes it onto the left ventricle for pumping to the organs of the body, including the muscles. Oxygen is thus delivered to the tissues and then the cycle repeats, more than 50,000 times per day! The left and right atria work in unison during heart filling (diastole), and the left and right ventricles work in unison during evacuation of blood from the heart (systole). Murmurs, often detected by veterinary surgeons when listening to hearts, are either caused by normal forward blood flow through the heart or by backflow leakage across the valves within the heart (regurgitation). Many of these murmurs are not a cause for concern, although some regurgitant murmurs are more severe and can cause problems with heart function. Similarly most heart rhythm abnormalities are innocuous and do not affect performance while others are more serious. In some horses, due to suspicion by a veterinary surgeon of a more significant problem, extensive evaluation of the heart is required; echocardiography is one of the key tools for diagnostic evaluation of the heart to assess the impact of any problems on athletic performance.

Image taken from the right side of the horse. Biplane views are on the left (4 chamber standard long axis view at top, short axis view at the bottom of the picture) and 3DE image on the right of the picture. In real-time the image can be manipulated as the heart is beating to visualise the cardiac structures from different angles. RV = right ventricle, TV = tricuspid valve, RA = right atrium, LV = left ventricle, MV = mitral valve, LA = left atrium.
Real-time three-dimensional echocardiography (3DE) is an exciting new tool that has recently become available in equine medicine and may shed light on important heart problems in horses, including those that cause poor performance. Compared to standard two dimensional echocardiography (2DE), which evaluates a single scan plane, 3DE involves the simultaneous collection of multiple scan planes from the heart to create a pyramid of scan data. 3DE is preferable to 2DE because in theory it does not rely on geometric assumptions on chamber shape to calculate chamber volumes. Also assessment of heart architecture and function (including that of valves) is likely to be more accurate as the technique provides unlimited viewing planes. Finally, for assessment of regurgitant flow, this technique should also be better because the image can be manipulated to better assess the leaky flow from those valves. In humans, for certain heart volume and muscle mass measurements, 3DE is more comparable than 2DE to cardiac magnetic resonance imaging (MRI), which is the acknowledged gold standard. Unfortunately, owing to the significantly larger size of horses, there is currently no equipment available for equine cardiac MRI. Therefore, 3DE could provide the next best option for more detailed equine cardiac evaluation.
Mitral valve regurgitation for example is commonly encountered in the equine athlete and, while often of no consequence, in more severe cases, it may lead to poor performance. Pathological consequences are due to backflow leakage causing secondary left atrial volume overload, and this will lead to an increased likelihood of atrial fibrillation. Potential advantages of 3DE in this context are more accurate assessment of the degree of volume overload, the regurgitant orifice (i.e., size of the hole!), and the valve structure and motion. Mitral valve regurgitation can be easily confirmed by 2DE, however it can be more difficult to ascertain the cause and severity. With 3DE, the software allows manipulation and therefore anatomic evaluation of the valves from many angles including ‘face-on‘ views. This results in more detailed evaluation of subtle abnormal valve motion and confirmation of suspected findings, which can’t be reliably detected by 2DE - eg. mitral valve thickening, mitral valve prolapse or ruptured chordae tendineae as the cause of mitral valve disease. Geometric assumptions on volume are avoided as much more structural data is obtained.
A few specialist centres worldwide currently offer 3DE imaging for horses including the Equine Hospital at the Royal (Dick) School of Veterinary Studies, University of Edinburgh. In equine medicine we are still at an early stage of using 3DE as it is not validated in horses, therefore it is mostly used in research at the moment as opposed to routine diagnosis. As part of my research at Edinburgh, sponsored by the Horserace Betting and Levy Board, I have been assessing the left atrial volume using 3DE from thoroughbreds in training. One of my aims was to determine the variability of equine left atrial volume measurement using a special 3DE software analysis package to see how much variation there was between successive 3DE measurements by the same person. Forty-four National Hunt thoroughbreds in training were scanned to obtain the 3DE views of this chamber. We then graded them to exclude images of reduced image quality so that we were only assessing good quality images of the left atrium. In total 24 horses were included—aged 4-9 yrs, weighing 411-534kg. I analysed the images retrospectively, after the horses were scanned. I didn’t include any horses with grade >3/6 heart murmurs. This was because we first need to validate 3DE with normal, healthy hearts. Random generated order measurements were obtained by a single person on four occasions. Real-time three-dimensional end-systolic (ESV) and end-diastolic (EDV) left atrial volumes were measured using 3DE software, and the results were then statistically analysed.
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
EIPH: An Australian Perspective with Worldwide Implications


By Ellie Crispe and Guy Lester
Exercise-induced pulmonary haemorrhage (EIPH) is a common disease of racehorses. The precise cause of EIPH is yet to be fully determined, but a well-accepted theory is that lung blood vessels rupture in response to the extremely high blood pressure and low airway pressure experienced during strenuous exercise. The barrier that separates the airway from the blood vessels is ultra-thin to facilitate the efficient exchange of gases, but this predisposes to breakage. The condition is most frequently described in Thoroughbred and Standardbred racehorses, but it has also been identified in racing Appaloosas and Quarter Horses, as well as horses involved in other high intensity athletic activities, including showjumpers, 3-day eventers, barrel racers, steeplechasers and polo horses.
EIPH is not unique to horses and has been reported in human athletes, as well as racing greyhounds and camels. Our group at Murdoch University in Perth Australia has had an interest in EIPH, which has led to three recent publications in the Equine Veterinary Journal.1-3
How common is EIPH?

Blood from both nostrils—also known as epistaxis—is the most obvious manifestation of EIPH and occurs between 1.5 and 8.4/1000 race starts, varying with racing jurisdiction. Epistaxis represents a severe manifestation of EIPH, and basing surveys on its presence vastly underestimates the true prevalence of lung haemorrhage. There are several techniques used to diagnose EIPH, but endoscopy of the trachea 30-120 minutes after racing or galloping is a common and reliable method. Occurrence and severity of pulmonary haemorrhage is typically graded using a 0-4 scale. Using endoscopy, we reported a prevalence of EIPH post-race in Australian thoroughbreds racing on turf tracks of around 55%, with most positive horses having low to moderate volumes of blood in the trachea. EIPH is less common if horses are examined after trialling, and reduced further if examined after track gallops. The prevalence of EIPH increases when horses are examined on multiple occasions after racing, and in fact all horses in our research population that had seven monitored race-starts experienced EIPH on at least one occasion.


What is the effect of EIPH on race-day performance?
It is generally considered that EIPH has a negative impact on racing performance, but evidence for this assertion is surprisingly lacking. We performed 3,794 post-race endoscopy exams on over 1,500 Australian horses and reported that inferior race-day performance was limited to horses with severe EIPH (grades 3 and 4); this reflected only 6.3% of all examinations. Horses with the highest grades of EIPH (grade 4) were less likely to finish in the first three, finished further from the winner, were less likely to collect race earnings, were slower over the final stages of the race, and were more likely to be overtaken by other competitors in the home straight than horses without EIPH. Interestingly, horses with EIPH grade 1 or 2 were more likely to overtake others in the home straight, compared to horses without EIPH (grade 0).

It is highly unlikely that low-grade EIPH (grade 1 or 2) confers an athletic advantage; a plausible explanation is that horses that are ridden competitively to the finish are functioning at their maximal physiological limit, compared to horses that are eased up, and overtaken, during the finishing stages of the race because they are not in prize contention or are affected by interference in the home straight. Another interesting finding was that horses with moderate to severe EIPH (grades 3 or 4) raced the early and mid-sections of the race faster than horses without EIPH. It is possible that these horses reach the breaking threshold of the small lung blood vessels at an earlier stage in the race compared to horses that start the race slower, compounding the severity thereafter. A study of barrel racing horses reported that horses with the most severe grade of EIPH were faster than horses without EIPH, a finding which may also reflect this rapid acceleration increasing the risk of EIPH. It may be wise for trainers to instruct jockeys riding horses with a history of moderate to severe EIPH to refrain from racing in this manner.
What is the effect of a one-off diagnosis of EIPH over a horse’s career?…