EIPH - could there be links to sudden death and pulmonary haemorrhage?
Dr Peter W. Physick-Sheard, BVSc, FRCVS, explores preliminary research and hypotheses, being conducted by the University of Guelph, to see if there is a possibility that these conditions are linked and what this could mean for future management and training of thoroughbreds.

"World's Your Oyster,” a three-year-old thoroughbred mare, presented at the veterinary hospital for clinical examination. She won her maiden start as a two-year-old and placed once in two subsequent starts. After training well as a three-year-old, she failed to finish her first start, easing at the top of the stretch, and was observed to fade abruptly during training. Some irregularity was suspected in heart rhythm after exercise. Thorough clinical examination, blood work, ultrasound of the heart and an ECG during rest and workout revealed nothing unusual.
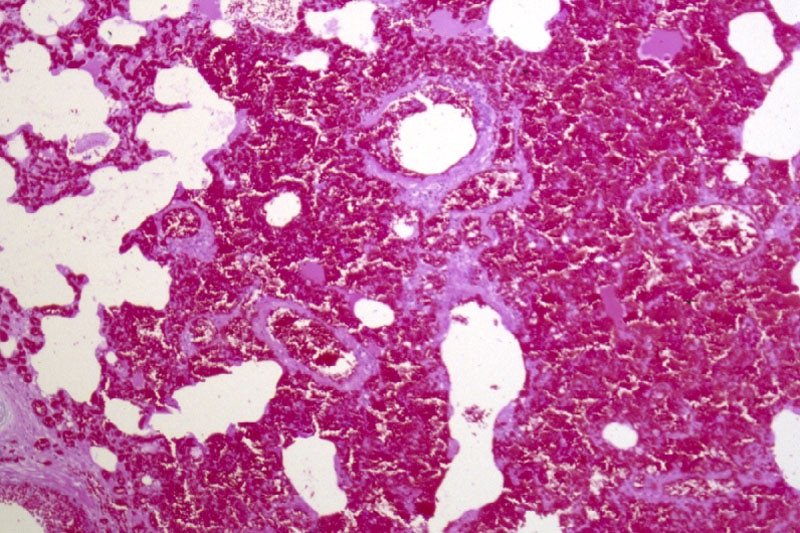
Returning to training, Oyster placed in six of her subsequent eight starts, winning the last two. She subsequently died suddenly during early training as a four-year-old. At post-mortem, diagnoses of pulmonary haemorrhage and exercise-induced pulmonary haemorrhage were established—a very frustrating and unfortunate outcome.

Across the racing world, a case like this probably occurs daily. Anything that can limit a horse's ability to express its genetic potential is a major source of anxiety when training. The possibility of injury and lameness is the greatest concern, but a close second is respiratory disease, with bleeding from the lungs (most often referred to as exercise induced pulmonary [lung] haemorrhage or EIPH) being high on the list.
EIPH is thought to occur in as many as 85 percent of racehorses, and may initially be very mild without obvious clinical consequences. In some cases it can be associated with haemorrhage of sufficient severity for blood to appear at the nostrils, even at first occurrence. In many racing jurisdictions this is a potentially career-ending problem. In these horses, an impact on performance is unquestionable. Bleeding from the lungs is the reason for the existence of ‘Lasix programs,’ involving pre-race administration of a medication considered to reduce haemorrhage. Such programs are controversial—the justifications for their existence ranging from addressing welfare concerns for the horse to dealing with the performance impacts.
Much less frequently encountered is heavy exercise-associated bleeding from the nostrils (referred to as epistaxis), which can sometimes be accompanied by sudden death, during or shortly after exercise. Some horses bleed heavily internally and die without blood appearing at the nostrils. Haemorrhage may only become obvious when the horse is lying on its side, or not until post-mortem. Affected animals do not necessarily have any history of EIPH, either clinically or sub-clinically. There is an additional group of rare cases in which a horse simply dies suddenly, most often very soon after work and even after a winning performance, and in which little to nothing clearly explains the cause on post-mortem. This is despite the fact most racing jurisdictions study sudden death cases very closely.
EIPH is diagnosed most often by bronchoscopy—passing an endoscope into the lung after work and taking a look. In suspected but mild cases, there may not be sufficient haemorrhage to be visible, and a procedure called a bronchoalveolar lavage is performed. The airways are rinsed and fluid is collected and examined microscopically to identify signs of bleeding. Scoping to confirm diagnosis is usually a minimum requirement before a horse can be placed on a Lasix program.
Are EIPH, severe pulmonary haemorrhage and sudden death related? Are they the same or different conditions?
At the University of Guelph, we are working on the hypothesis that most often they are not different—that it’s degrees of the same condition, or closely related conditions perhaps with a common underlying cause. We see varying clinical signs as being essentially a reflection of severity and speed of onset of underlying problems.

Causes in individual cases may reflect multiple factors, so coming at the issues from several different directions, as is the case with the range of ongoing studies, is a good way to go so long as study subjects and cases are comparable and thoroughly documented. However, starting from the hypothesis that these may all represent basically the same clinical condition, we are approaching the problem from a clinical perspective, which is that cardiac dysfunction is the common cause.
Numerous cardiac disorders and cellular mechanisms have the potential to contribute to transient or complete pump (heart) failure. However, identifying them as potential disease candidates does not specifically identify the role they may have played, if any, in a case of heart failure and in lung haemorrhage; it only means that they are potential primary underlying triggers. It isn't possible for us to be right there when a haemorrhage event occurs, so almost invariably we are left looking at the outcome—the event of interest has passed. These concerns influence the approach we are taking.
Background
The superlative performance ability of a horse depends on many physical factors:
Huge ventilatory (ability to move air) and gas exchange capacity
Body structure including limb length and design - allows it to cover ground rapidly with a long stride
Metabolic adaptations - supports a high rate of energy production by burning oxygen, tolerance of severe metabolic disruptions toward the end of race-intensity effort
High cardiovascular capacity - allows the average horse to pump roughly a brimming bathtub of blood every minute
At race intensity effort, these mechanisms, and more, have to work in coordination to support performance. There is likely not much reserve left—two furlongs (400m) from the winning post—even in the best of horses. There are many wild cards, from how the horse is feeling on race day to how the race plays out; and in all horses there will be a ceiling to performance. That ceiling—the factor limiting performance—may differ from horse to horse and even from day to day. There’s no guarantee that in any particular competition circumstances will allow the horse to perform within its own limitations. One of these factors involves the left side of the heart, from which blood is driven around the body to the muscles.
A weak link - filling the left ventricle
The cardiovascular system of the horse exhibits features that help sustain a high cardiac output at peak effort. The feature of concern here is the high exercise pressure in the circulation from the right ventricle, through the lungs to the left ventricle. At intense effort and high heart rates, there is very little time available to fill the left ventricle—sometimes as little as 1/10 of a second; and if the chamber cannot fill properly, it cannot empty properly and cardiac output will fall. The circumstances required to achieve adequate filling include the readiness of the chamber to relax to accept blood—its ‘stiffness.’ Chamber stiffness increases greatly at exercise, and this stiffened chamber must relax rapidly in order to fill. That relaxation seems not to be sufficient on its own in the horse at high heart rates. Increased filling pressure from the circulation draining the lungs is also required. But there is a weak point: the pulmonary capillaries.

These are tiny vessels conducting blood across the lungs from the pulmonary artery to the pulmonary veins. During this transit, all the gas exchange needed to support exercise takes place. The physiology of other species tells us that the trained lung circulation achieves maximum flow (equivalent to cardiac output) by reducing resistance in those small vessels. This process effectively increases lung blood flow reserve by, among other things, dilating small vessels. Effectively, resistance to the flow of blood through the lungs is minimised. We know this occurs in horses as it does in other species; yet in the horse, blood pressure in the lungs still increases dramatically at exercise.
If this increase is not the result of resistance in the small vessels, it must reflect something else, and that appears to be resistance to flow into the left chamber. This means the entire lung circulation is exposed to the same pressures, including the thin-walled capillaries. Capillaries normally work at quite low pressure, but in the exercising horse, they must tolerate very high pressures. They have thin walls and little between them, and the air exchange sacs in the lung. This makes them vulnerable. It's not surprising they sometimes rupture, resulting in lung haemorrhage.

Recent studies identified changes in the structure of small veins through which the blood flows from the capillaries and on toward the left chamber. This was suspected to be a pathology and part of the long-term consequences of EIPH, or perhaps even part of the cause as the changes were first identified in EIPH cases. It could be, however, that remodelling is a normal response to the very high blood flow through the lungs—a way of increasing lung flow reserve, which is an important determinant of maximum rate of aerobic working.
The more lung flow reserve, the more cardiac output and the more aerobic work an animal can perform. The same vein changes have been observed in non-racing horses and horses without any history or signs of bleeding. They may even be an indication that everything is proceeding as required and a predictable consequence of intense aerobic training. On the other hand, they may be an indication in some horses that the rate of exercise blood flow through their lungs is a little more than they can tolerate, necessitating some restructuring. We have lots to learn on this point.
If the capacity to accommodate blood flow through the lungs is critical, and limiting, then anything that further compromises this process is likely to be of major importance. It starts to sound very much as though the horse has a design problem, but we shouldn't rush to judgement. Horses were probably not designed for the very intense and sustained effort we ask of them in a race. Real-world situations that would have driven their evolution would have required a sprint performance (to avoid ambush predators such as lions) or a prolonged slower-paced performance to evade predators such as wolves, with only the unlucky victim being pushed to the limit and not the entire herd.
Lung blood flow and pulmonary oedema
There is another important element to this story. High pressures in the capillaries in the lung will be associated with significant movement of fluid from the capillaries into lung tissue spaces. This movement in fact happens continuously at all levels of effort and throughout the body—it's a normal process. It's the reason the skin on your ankles ‘sticks’ to the underlying structures when you are standing for a long time. So long as you keep moving a little, the lymphatic system will draw away the fluid.
In a diseased lung, tissue fluid accumulation is referred to as pulmonary oedema, and its presence or absence has often been used to help characterise lung pathologies. The lung lymphatic system can be overwhelmed when tissue fluid is produced very rapidly. When a horse experiences sudden heart failure, such as when the supporting structures of a critical valve fail, one result is massive overproduction of lung tissue fluid and appearance of copious amounts of bloody fluid from the nostrils.
The increase in capillary pressure under these conditions is as great as at exercise, but the horse is at rest. So why is there no bloody fluid in the average, normal horse after a race? It’s because this system operates very efficiently at the high respiratory rates found during work: tissue fluid is pumped back into the circulation, and fluid does not accumulate. The fluid is pumped out as quickly as it is formed. An animal’s level of physical activity at the time problems develop can therefore make a profound difference to the clinical signs seen and to the pathology.
Usual events with unusual consequences
If filling the left ventricle and the ability of the lungs to accommodate high flow at exercise are limiting factors, surely this affects all horses. So why do we see such a wide range of clinical pictures, from normal to subclinical haemorrhage to sudden death?
Variation in contributing factors such as type of horse, type and intensity of work, sudden and unanticipated changes in work intensity, level of training in relation to work and the presence of disease states are all variables that could influence when and how clinical signs are seen, but there are other considerations.
Although we talk about heart rate as a fairly stable event, there is in fact quite a lot of variation from beat to beat. This is often referred to as heart rate variability. There has been a lot of work performed on the magnitude of this variability at rest and in response to various short-term disturbances and at light exercise in the horse, but not a lot at maximal exercise. Sustained heart rate can be very high in a strenuously working horse, with beats seeming to follow each other in a very consistent manner, but there is in fact still variation.
Some of this variation is normal and reflects the influence of factors such as respiration. However, other variations in rate can reflect changes in heart rhythm. Still other variations may not seem to change rhythm at all but may instead reflect the way electrical signals are being conducted through the heart.
These may be evident from the ECG but would not appear abnormal on a heart rate monitor or when listening. These variations, whether physiologic (normal) or a reflection of abnormal function, will have a presently, poorly understood influence on blood flow through the lungs and heart—and on cardiac filling. Influences may be minimal at low rates, but what happens at a heart rate over 200 and in an animal working at the limits of its capacity?
Normal electrical activation of the heart follows a pattern that results in an orderly sequence of heart muscle contraction, and that provides optimal emptying of the ventricles. Chamber relaxation complements this process.
An abnormal beat or abnormal interval can compromise filling and/or emptying of the left ventricle, leaving more blood to be discharged in the next cycle and back up through the lungs, raising pulmonary venous pressure. A sequence of abnormal beats can lead to a progressive backup of blood, and there may not be the capacity to hold it—even for one quarter of a second, a whole cardiac cycle at 240 beats per minute.
For a horse that has a history of bleeding and happens to be already functioning at a very marginal level, even minor disturbances in heart rhythm might therefore have an impact. Horses with airway disease or upper airway obstructions, such as roarers, might find themselves in a similar position. An animal that has not bled previously might bleed a little, one that has a history of bleeding may start again, or a chronic bleeder may worsen.
Relatively minor disturbances in cardiac function, therefore, might contribute to or even cause EIPH. If a horse is in relatively tough company or runs a hard race, this may also contribute to the onset or worsening of problems. Simply put, it's never a level playing field if you are running on the edge.
Severe bleeding
It has been suspected for many years that cases of horses dying suddenly at exercise represent sudden-onset cardiac dysfunction—most likely a rhythm disturbance. If the rhythm is disturbed, the closely linked and carefully orchestrated sequence of events that leads to filling of the left ventricle is also disturbed. A disturbance in cardiac electrical conduction would have a similar effect, such as one causing the two sides of the heart to fall out of step, even though the rhythm of the heart may seem normal.
The cases of horses that bleed profusely at exercise and even those that die suddenly without any post-mortem findings can be seen to follow naturally from this chain of events. If the changes in heart rhythm or conduction are sufficient, in some cases to cause massive pulmonary haemorrhage, they may be sufficient in other cases to cause collapse and death even before the horse has time to exhibit epistaxis or even clear evidence of bleeding into the lungs.

EIPH and dying suddenly
If these events are (sometimes) related, why is it that some horses that die of pulmonary haemorrhage with epistaxis do not show evidence of chronic EIPH? This is one of those $40,000 questions. It could be that young horses have had limited opportunity to develop chronic EIPH; it may be that we are wrong and the conditions are entirely unrelated. But it seems more likely that in these cases, the rhythm or conduction disturbance was sufficiently severe and/or rapid in onset to cause a precipitous fall in blood pressure with the animal passing out and dying rapidly.
In this interpretation of events, the missing link is the heart. There is no finite cutoff at which a case ceases to be EIPH and becomes pulmonary haemorrhage. Similarly, there is no distinct point at which any case ceases to be severe EIPH and becomes EAFPH (exercise-associated fatal pulmonary haemorrhage). In truth, there may simply be gradation obscured somewhat by variable definitions and examination protocols and interpretations.
The timing of death
It seems from the above that death should most likely take place during work, and it often does, but not always. It may occur at rest, after exercise. Death ought to occur more often in racing, but it doesn't.
The intensity of effort is only one factor in this hypothesis of acute cardiac or pump failure. We also have to consider factors such as when rhythm disturbances are most likely to occur (during recovery is a favourite time) and death during training is more often a problem than during a race.
A somewhat hidden ingredient in this equation is possibly the animal's level of emotional arousal, which is known to be a risk factor in humans for similar disturbances. There is evidence that emotions/psychological factors might be much more important in horses than previously considered. Going out for a workout might be more stimulating for a racehorse than a race because before a race, there is much more buildup and the horse has more time to adequately warm up psychologically. And then, of course, temperament also needs to be considered. These are yet further reasons that we have a great deal to learn.

Our strategy at the University of Guelph
These problems are something we cannot afford to tolerate, for numerous reasons—from perspectives of welfare and public perception to rider safety and economics. Our aim is to increase our understanding of cardiac contributions by identifying sensitive markers that will enable us to say with confidence whether cardiac dysfunction—basically transient or complete heart failure—has played a role in acute events.
We are also looking for evidence of compromised cardiac function in all horses, from those that appear normal and perform well, through those that experience haemorrhage, to those that die suddenly without apparent cause. Our hope is that we can not only identify horses at risk, but also focus further work on the role of the heart as well as the significance of specific mechanisms. And we hope to better understand possible cardiac contributions to EIPH in the process. This will involve digging deeply into some aspects of cellular function in the heart muscle, the myocardium of the horse, as well as studying ECG features that may provide insight and direction.
Fundraising is underway to generate seed money for matching fund proposals, and grant applications are in preparation for specific, targeted investigations. Our studies complement those being carried out in numerous, different centres around the world and hopefully will fill in further pieces of the puzzle. This is, indeed, a huge jigsaw, but we are proceeding on the basis that you can eat an elephant if you're prepared to process one bite at a time.
How can you help? Funding is an eternal issue. For all the money that is invested in horses there is a surprisingly limited contribution made to research and development—something that is a mainstay of virtually every other industry; and this is an industry.
Look carefully at the opportunities for you to make a contribution to research in your area. Consider supporting studies by making your experience, expertise and horses available for data collection and minimally invasive procedures such as blood sampling.
Connect with the researchers in your area and find out how you can help. Watch your horses closely and contemplate what they might be telling you—it's easy to start believing in ourselves and to stop asking questions. Keep meticulous records of events involving horses in your care— you never know when you may come across something highly significant. And work with researchers (which often includes track practitioners) to make your data available for study.
Remember that veterinarians and university faculty are bound by rules of confidentiality, which means what you tell them should never be ascribed to you or your horses and will only be used without any attribution, anonymously. And when researchers reach out to you to tell you what they have found and to get your reactions, consider actually attending the sessions and participating in the discussion; we can all benefit—especially the ultimate beneficiary which should be the horse. We all have lots to learn from each other, and finding answers to our many challenges is going to have to be a joint venture.
Finally, this article has been written for anybody involved in racing to understand, but covering material such as this for a broad audience is challenging. So, if there are still pieces that you find obscure, reach out for help in interpretation. The answers may be closer than you think!
Oyster
And what about Oyster? Her career was short. Perhaps, had we known precisely what was going on, we might have been able to treat her, or at least withdraw her from racing and avoid a death during work with all the associated dangers—especially to the rider and the associated welfare concerns.
Had we had the tools, we might have been able to confirm that whatever the underlying cause, she had cardiac problems and was perhaps predisposed to an early death during work. With all the other studies going on, and knowing the issue was cardiac, we might have been able to target her assessment to identify specific issues known to predispose.
In the future, greater insight and understanding might allow us to breed away from these issues and to better understand how we might accommodate individual variation among horses in our approaches to selection, preparation and competition. There might be a lot of Oysters out there!
For further information about the work being undertaken by the University of Guelph
Contact - Peter W. Physick-Sheard, BVSc, FRCVS.
Professor Emeritus, Ontario Veterinary College, University of Guelph - pphysick@uoguelph.ca
Research collaborators - Dr Glen Pyle, Professor, Department of Biomedical Sciences, University of Guelph - gpyle@uoguelph.ca
Dr Amanda Avison, PhD Candidate, Department of Biomedical Sciences, University of Guelph. ajowett@uoguelph.ca
References
Caswell, J.I. and Williams K.J. (2015), Respiratory System, In ed. Maxie, M. Grant, 3 vols., 6th edn., Jubb, Kennedy and Palmer’s Pathology of Domestic Animals, 2; London: Elsevier Health Sciences, 490-91.
Hinchcliff, KW, et al. (2015), Exercise induced pulmonary hemorrhage in horses: American College of Veterinary Internal Medicine consensus statement, J Vet Intern Med, 29 (3), 743-58.
Rocchigiani, G, et al. (2022), Pulmonary bleeding in racehorses: A gross, histologic, and ultrastructural comparison of exercise-induced pulmonary hemorrhage and exercise-associated fatal pulmonary hemorrhage, Vet Pathol, 16:3009858221117859. doi: 10.1177/03009858221117859. Online ahead of print.
Manohar, M. and T. E. Goetz (1999), Pulmonary vascular resistance of horses decreases with moderate exercise and remains unchanged as workload is increased to maximal exercise, Equine Vet. J., (Suppl.30), 117-21.
Vitalie, Faoro (2019), Pulmonary Vascular Reserve and Aerobic Exercise Capacity, in Interventional Pulmonology and Pulmonary Hypertension, Kevin, Forton (ed.), (Rijeka: IntechOpen), Ch. 5, 59-69.
Manohar, M. and T. E. Goetz (1999), Pulmonary vascular resistance of horses decreases with moderate exercise and remains unchanged as workload is increased to maximal exercise, Equine Vet. J., (Suppl.30), 117-21.
Can nutrition influence EIPH? - alternative and supportive therapies as trainers seek to find other means of reducing the risk or severity of EIPH

By Catherine Rudenko
EIPH (exercise-induced pulmonary haemorrhage) was first identified in racehorses in the 16th century. Since this time, the focus has been on mitigating the haemorrhage. Management of EIPH largely revolves around the use of furosemide, dependent of jurisdiction, may or may not be used on the day of racing. Alternative and supportive therapies are becoming increasingly popular as trainers seek to find other means of reducing the risk or severity of EIPH.
Nutrition and plant-based approaches are part of an alternative management program. Whilst research is somewhat limited, the studies available are promising, and no doubt more work will be done as using furosemide becomes more restricted. There are several directions in which nutrition can influence risk for EIPH, including inflammatory response, blood coagulation, cell membrane structure, hypotension and reducing known lung irritants.

The various approaches are all supportive, working on altering an element of risk associated with the condition. Some are more direct than others, focusing on the effect on red blood cells, whilst others work on some of the broader lung health issues such as reducing mucus or environmental irritants.
None are competitive with each other, and there may be an advantage to a ‘cocktail’ approach where more than one mode of action is employed. This is a common practice with herbal-based supplements where the interactive effects between herbs are known to improve efficacy.
Cell membrane
The red blood cell membrane—the semipermeable layer surrounding the cell—is made up of lipids and proteins. The makeup of this membrane, particularly the lipid fraction, appears to be modifiable in response to dietary fatty acids. Researchers feeding 50mls of fish oil found a significant increase in the percentage of omega-3’s in the cell membrane.
Essential fatty acids (EFA’s), omega 3 and omega 6, are important cell membrane components and determine cellular membrane fluidity. Fluidity of a cell membrane is important, particularly when pressure increases, as a cell membrane lacking in fluidity is more likely to break. A cell that can deform, effectively changing rather than breaking, has an advantage and is linked with improved exercise performance in human studies. Inclusion of fish oil in the diet increases the ability of red blood cells to deform.
Kansas State University investigated the effect of omega supplementation on 10 thoroughbreds over a five-month period. The diet was supplemented with either EPA and DHA combined, or DHA on its own. EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) are specific forms of omega-3 fatty acids commonly found in oily fish. When supplementing the diet with both EPA and DHA, a reduction in EIPH was seen at 83 days and again at 145 days. Feeding DHA on its own did not produce an effect.
Fish oil contains both EPA and DHA and is readily available, although the smell can be off-putting to both horse and human. There are flavoured fish oils specifically designed for use in horses that overcome the aroma challenge and have good palatability.
Inflammatory response and oxidative stress

Kentucky Equine research results
Airway inflammation and the management of this inflammatory process is believed to be another pathway in which EIPH can be reduced. Omega-3 fatty acids are well evidenced for their effect in regulation of inflammation, and this mode of action along with effect on cell membrane fluidity is likely part of the positive result found by Kansas State University.
Kentucky Equine Research has investigated the effect of a specific fish oil on inflammatory response with horses in training. The study supplemented test horses with 60mls per day and found a significant effect on level of inflammation and GGT (serum gamma-glutamyl transferase). GGT is an enzyme that breaks down glutathione, an important antioxidant. As GGT rises, less glutathione is available to neutralise damaging free radicals, creating an environment for oxidative stress.
A horse’s red blood cells are more susceptible to oxidative stress than humans, and maintaining a healthy antioxidant status is important for function and maintenance of cell integrity.

Rosehip
Supplements for bleeders will often contain relatively high doses of antioxidants such as vitamin C and vitamin E to support antioxidant status in the horse and reduce risk of damage to cell membranes. Vitamin C has also been shown to benefit horses with recurrent airway obstruction and increase antibody response. Dose rates required for an effect range from 15-20g per day. If including high doses of vitamin C in the diet, it is important to note that any sudden withdrawal can have negative effects. Gradual withdrawal is needed to allow the body’s own mechanisms for vitamin C production to recognise and respond to the change in status.
Rosehips are natural potent antioxidants containing many active substances. Research into the effect of rosehips specifically on red blood cells has shown they have a high efficacy when assessing their ability to ameliorate cell damage.
Hypotensive herbs

Caucus carota – wild carrott
The essential oil of caucus carota species is a well-documented oil having a hypotensive, lowering of blood pressure effect along with antifungal properties. Its antifungal effects are noted against aspergillus species, a common cause of poor respiratory health. Allium sativum is also well known for its ability to lower blood pressure. An initial study (data unpublished) into the effects of these two plants along with herbs reported to alleviate mucus in the lungs has shown promising results in a group of horses in training.
Prolonged blood coagulation
As prolonged blood coagulation is cited as a possible factor for EIPH, herbal products that are noted for their ability to enhance coagulation are in certain parts of the world widely used as part of managing EIPH. …
CLICK HERE to return to issue contents


ISSUE 58 (PRINT)
$6.95
ISSUE 58 (DIGITAL)
$3.99
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Four issue subscription - ONLY $24.95
Bleeders - facts- fiction - future - treatment - of exercise-induced haemorrhages

By Dr. David Marlin
We are now approaching half a century since Bob Cook pioneered the use of the flexible fibreoptic endoscope, which allowed examination of the respiratory tract in the conscious horse. One of the important outcomes of this technique was that it opened the door to the study of “bleeding” or exercise-induced pulmonary hemorrhage (EIPH).
But nearly 50 years on the irony is perhaps that whilst we have become good at describing the prevalence of EIPH and some of the factors that appear to increase the severity of EIPH within individual horses, we still lack a clear understanding of the condition and how to manage it.
I use the term manage rather than treat or prevent as our knowledge of EIPH must show us that EIPH cannot be stopped entirely; it is a consequence of intense exercise. The other irony is that in the past 50 years, by far the majority of research into the management of EIPH has focused on the use of the diuretic furosemide. Whilst we have good evidence from controlled studies that furosemide reduces the severity of EIPH on a single occasion, we still lack good evidence to suggest that furosemide is effective when used repeatedly during training and or racing; and there is also evidence to the contrary. Let’s review some basic facts about EIPH, which should not be contentious.
• EIPH is the appearance of blood in the airways associated with exercise.
• EIPH occurs as a result of moderate to intense exercise. In fact, EIPH has been found after trotting when deep lung wash (bronchoalveolar lavage or BAL) is done after exercise.
• EIPH most often involves the smallest blood vessels (capillaries) but can sometimes and less commonly be due to the rupture of larger blood vessels.
• The smallest blood vessels are extremely thin. Around 1/100th the thickness of a human hair. But this extremely thin membrane is also what allows racehorses such as Thoroughbreds, Standardbreds and Arabs to use oxygen at such a high rate and is a major reason for their athleticism.
• EIPH is a progressive condition. The chance of seeing blood in the trachea after exercise increases with time in racing.
• EIPH is variable over time, even when horses are scoped after the same type of work.
• If you ‘scope a horse after three gallops in a row, you can expect to see blood in the trachea on at least one occasion.
• EIPH damage to the lungs starts at the back and top, and over time moves forward and down and is approximately symmetrical.
• Following EIPH the lung becomes fibrotic (as scar tissue), stiffer and does not work as well. The iron from the blood is combined with protein and stored permanently in the lung tissue where it can cause inflammation.
• High blood pressure within the lung is a contributing factor in EIPH. Horses with higher blood pressure appear to suffer worse EIPH.
• There is also evidence that upper airway resistance and breathing pattern can play a role in EIPH.
• Airway inflammation and poor air quality may increase the severity of EIPH within individual horses.
• Increasing severity of EIPH appears to have an increasing negative effect on performance.
• Visible bleeding (epistaxis) has a very clear and marked negative effect on performance. In order to make progress in the management of EIPH (i.e., to minimize the severity of EIPH in each individual), there are certain steps that trainers can take based on the information we have to date. These include:
• Ensuring good air quality in stables • Regular respiratory examination and treatment of airway inflammation • Reduced intensity of training during periods of treatment for moderate to severe airway inflammation
• Extended periods of rest and light work with a slower return to work for horses following viral infection
• Addressing anything that increases upper airway resistance (e.g., roaring, gurgling)
• Avoiding intense work in cold weather
• Avoiding extremes of going

• Limiting number of training days in race preparation and increasing interval between races.
FUTURE OPPORTUNITIES IN UNDERSTANDING AND MANAGING EIPH
We have to accept EIPH as a normal consequence of intense exercise in horses. Our aim should be to reduce the severity to a minimum in each individual horse. However, there are areas in which we still need a much greater scientific understanding.
What actually causes the capillaries to leak or rupture?
If you ask any vet, scientist or informed trainer what is the cause of EIPH, they will give the phrase “pulmonary capillary stress-failure”. But this is simply a description of what happens—NOT an explanation or a mechanism. EIPH and pulmonary capillary stress-failure are both descriptions of what’s happening. We know high blood pressure makes the capillaries stiff. But what makes them actually rupture? A balloon filled with water may be distended and under a lot of stress. But a pin prick will actually make it burst. The pin is the cause.
Assessing EIPH
At present the most common way to assess the severity of EIPH in horses in training and racing is by ‘scoping 30-40 minutes after exercise and scoring the amount of blood in the trachea. This is a crude method, and when we see a horse that has a score of 1 after one gallop and a 3 after the next gallop, we don’t know whether this is due to differences in how quickly the blood has moved from the periphery of the lung into the trachea or due to a true difference in the amount of bleeding. We know our ‘scoping scores vary from gallop to gallop; we just don’t know why.BAL (deep lung wash) is not the answer either. It will pick up blood when there is none to be seen in the trachea (i.e., it’s a more sensitive technique), but with BAL we are looking atrelatively small areas of the lung. What we need is a technique that will allow us to image the whole lung and map the blood that is in the airways and not in the blood vessels so we can assess volume and distribution of hemorrhage.
Furosemide is not the answer


A number of well-conducted and well-written scientific studies have shown conclusively that furosemide is effective in reducing the severity of EIPH in individual horses when used ONE time! We lack convincing studies that prove furosemide works as well when used one to two times a week for two to three months. In fact, several studies suggest that furosemide becomes less effective with regular use, such as the return to previous performance of horses after initial racing and improved performance on furosemide. In human medicine, repetitive administration of furosemide induces short-term (braking phenomenon, acute diuretic resistance) and longterm (chronic diuretic resistance) tolerance (i.e., if you give the same dose repeatedly, the body becomes tolerant and you get less and less urine production). A study in horses from Michigan State University in 2017 showed horses develop tolerance to furosemide. Why, when we have had nearly 50 years of research into EIPH with more published studies devoted to furosemide than any other aspect, do we still not know if furosemide is effective when used on a regular basis?
Is EIPH really blood?…
CLICK HERE to return to issue content


BUY THIS ISSUE IN PRINT OR DOWNLOAD
ISSUE 56 (PRINT)
$6.95
ISSUE 56 (DIGITAL)
$3.99
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Four issue subscription - PRINT & ONLINE - ONLY $24.95

Australian EIPH report - new research on the impact of EIPH from an Australian perspective but with worldwide implications

By Guy Lester and Ellie Crispe
Exercise-induced pulmonary hemorrhage (EIPH) is a common disease of racehorses. The precise cause of EIPH is yet to be fully determined, but a well-accepted theory is that lung blood vessels rupture in response to the extremely high blood pressure and low airway pressure experienced during strenuous exercise. The barrier that separates the airway from the blood vessels is ultra-thin to facilitate the efficient exchange of gases, but this predisposes to breakage. The condition is most frequently described in Thoroughbred and Standardbred racehorses, but it has also been identified in racing Appaloosas and Quarter Horses, as well as horses involved in other high-intensity athletic activities, including showjumpers, 3-day eventers, barrel racers, steeplechasers and polo horses.
EIPH is not unique to horses and has been reported in human athletes, as well as racing greyhounds and camels. Our group at Murdoch University in Perth, Australia has had an interest in EIPH, which has led to three recent publications in the Equine Veterinary Journal.1-3
How common is EIPH?

Blood from both nostrils—also known as epistaxis—is the most obvious manifestation of EIPH and occurs between 1.5 and 8.4/1000 race starts, varying with racing jurisdiction. Epistaxis represents a severe manifestation of EIPH, and basing surveys on its presence vastly underestimates the true prevalence of lung hemorrhage. There are several techniques used to diagnose EIPH, but endoscopy of the trachea 30-120 minutes after racing or galloping is a common and reliable method. Occurrence and severity of pulmonary hemorrhage is typically graded using a 0-4 scale. Using endoscopy, we reported a prevalence of EIPH post-race in Australian Thoroughbreds racing on turf tracks of around 55%, with most positive horses having low to moderate volumes of blood in the trachea. EIPH is less common if horses are examined after trialing and reduced further if examined after track gallops. The prevalence of EIPH increases when horses are examined on multiple occasions after racing; and in fact, all horses in our research population that had seven monitored race-starts experienced EIPH on at least one occasion.
What is the effect of EIPH on race-day performance?
It is generally considered that EIPH has a negative impact on racing performance, but evidence for this assertion is surprisingly lacking. We performed 3,794 post-race endoscopy exams on over 1,500 Australian horses and reported that inferior race-day performance was limited to horses with severe EIPH (grades 3 and 4); this reflected only 6.3% of all examinations. Horses with the highest grades of EIPH (grade 4) were less likely to finish in the first three, finished further from the winner, were less likely to collect race earnings, were slower over the final stages of the race, and were more likely to be overtaken by other competitors in the home straight than horses without EIPH. Interestingly, horses with EIPH grade 1 or 2 were more likely to overtake others in the home straight, compared to horses without EIPH (grade 0). It is highly unlikely that low-grade EIPH (grade 1 or 2) confers an athletic advantage; a plausible explanation is that horses that are ridden competitively to the finish are functioning at their maximal physiological limit, compared to horses that are eased up and overtaken during the finishing stages of the race because they are not in prize contention or are affected by interference in the home straight. Another interesting finding was that horses with moderate to severe EIPH (grades 3 or 4) raced the early and mid-sections of the race faster than horses without EIPH. It is possible that these horses reach the breaking threshold of the small lung blood vessels at an earlier stage in the race compared to horses that start the race slower, compounding the severity thereafter. A study of barrel racing horses reported that horses with the most severe grade of EIPH were faster than horses without EIPH, a finding which may also reflect this rapid acceleration increasing the risk of EIPH. It may be wise for trainers to instruct jockeys riding horses with a history of moderate to severe EIPH to refrain from racing in this manner.
What is the effect of a one-off diagnosis of EIPH over a horse’s career?
A pattern of increasing endoscopic EIPH severity over a racehorse’s career is suspected but has not been proven. Another Australian research group examined 744 Thoroughbreds post-race with endoscopy, looked back 12 years later and compared EIPH score to their career performance. There was no association between any grade of EIPH and career duration, lifetime earnings, or the number of wins or places. These observations led to the conclusion that a one-off diagnosis of EIPH is an unreliable predictor of overall career performance.
Is EIPH a progressive disease?

EIPH is typically described as a progressive disease, but again, evidence is lacking. In our Australian Thoroughbred population, EIPH scores were often erratic from one race start to the next, especially as the EIPH severity increases. We were able to identify factors which were associated with change in EIPH score from one race start to another and which might help manage horses that are prone to EIPH. Increasing the number of days between races was associated with a transition from a higher to a lower grade of EIPH and racing in cooler weather was associated with a transition from a lower to a higher EIPH grade at the next observation. There are also likely to be unmeasured intra-horse and race factors that could also account for the variation in EIPH scores from one race start to another. Although in individual horses, EIPH severity can differ from race to race, from a population perspective, we concluded that EIPH is a mildly progressive condition.
What are the risk factors for EIPH?
Several investigators have found an association between temperature and EIPH. Cold weather on race day increases the chances of diagnosing EIPH and increases the chances of diagnosing more severe grades of EIPH. Furthermore, for horses that previously had no or only mild EIPH, racing in colder weather was more likely to be associated with a worsening of EIPH grade at the next observation. The reason that EIPH worsens with cold weather is unknown, but this phenomenon could mimic cold-induced pulmonary hypertension reported in other species. It may reflect the ambient temperature during training rather than specifically the temperature at the time of the race. Avoiding cold weather during training or racing may reduce the risk of EIPH in horses with a history of moderate to severe EIPH.
TO READ MORE —
BUY THIS ISSUE IN PRINT OR DOWNLOAD -
Triple Crown 2019, issue 52 (PRINT)
$6.95
Triple Crown 2019, issue 52 (DOWNLOAD)
$3.99
WHY NOT SUBSCRIBE?
DON'T MISS OUT AND SUBSCRIBE TO RECEIVE THE NEXT FOUR ISSUES!
Print & Online Subscription
From $24.95
Is EIPH beyond the scope of dietary change?

GET YOUR HANDS ON THIS ISSUE - VISIT OUR ONLINE SHOP HERE!
Are you a subscriber?
Don't miss out and subscribe to receive the print magazine now! CLICK HERE
Does bleeding affect performance? Results of a ten year study

CLICK ON THE IMAGE ABOVE TO READ ONLINE!
The 50 shades of gray in the EIPH and Salix debate
CLICK ON IMAGE TO READ ARTICLE
THIS ARTICLE FIRST APPEARED IN - NORTH AMERICAN TRAINER - ISSUE 25